

Outpatient labor induction-Exploring future potential by assessing eligibility in a historical cohort
- PMID: 38504457
- PMCID: PMC11103143
- DOI: 10.1111/aogs.14799
Outpatient labor induction-Exploring future potential by assessing eligibility in a historical cohort
Abstract
Introduction: Labor induction rates have increased over the last decades, and in many high-income countries, more than one in four labors are induced. Outpatient management of labor induction has been suggested in low-risk pregnancies to improve women's birth experiences while also promoting a more efficient use of healthcare resources. The primary aim of this paper was to assess the proportion of women in a historical cohort that would have been eligible for outpatient labor induction with oral misoprostol. Second, we wanted to report safety outcomes and assess efficacy outcomes for mothers and infants in pregnancies that met the criteria for outpatient care.
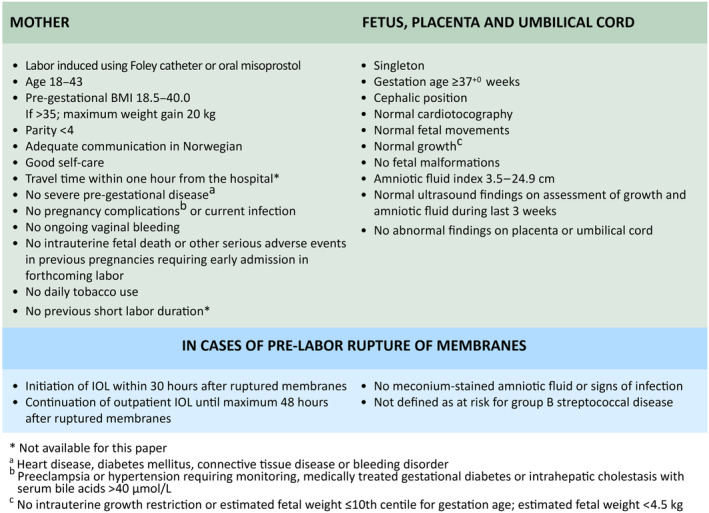
Material and methods: Criteria for outpatient labor induction with oral misoprostol were applied to a historical cohort of women with induction of labor at two Norwegian tertiary hospitals in the period January 1, through July 31, 2021. The criteria included low-risk women with an unscarred uterus expecting a healthy, singleton baby in cephalic position at term. The primary outcome was the proportion of women eligible for outpatient labor induction. Secondary outcomes included reasons for ineligibility and, for eligible women, safety and efficacy outcomes.
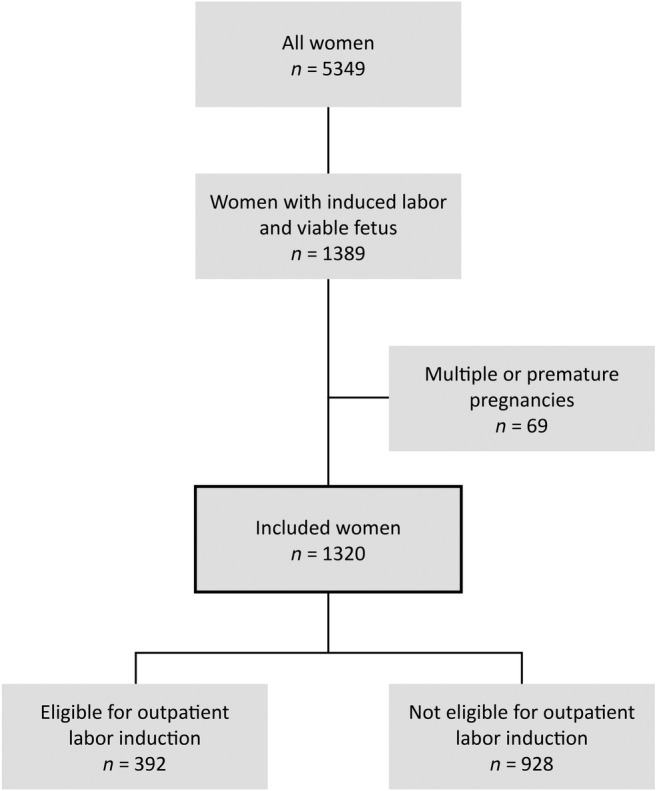
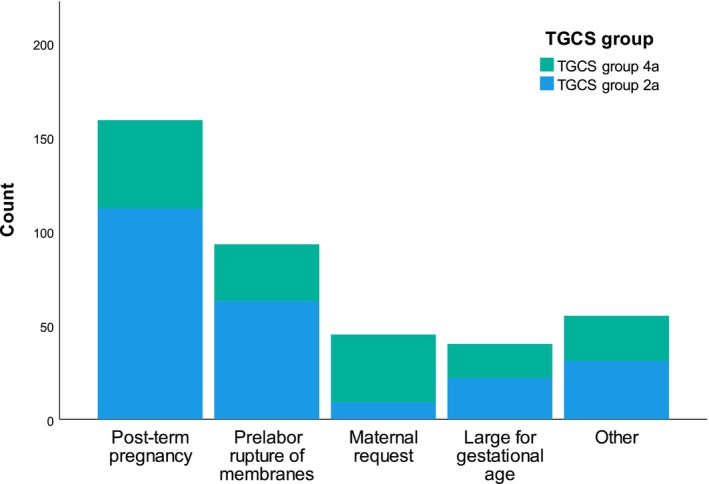
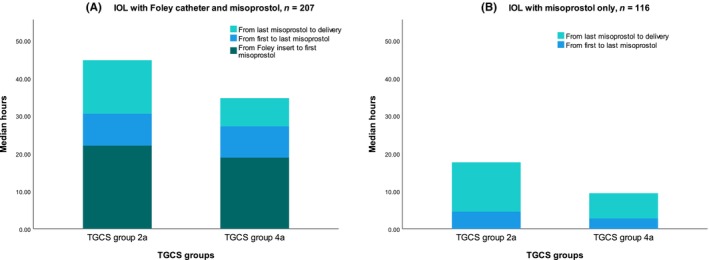
Results: Overall, 29.7% of the 1320 women who underwent labor induction in a singleton term pregnancy met the criteria for outpatient labor induction. We identified two serious adverse events that potentially could have occurred outside the hospital if the women had received outpatient care. The mean duration from initiation of labor induction to administration of the last misoprostol was 22.4 h. One in 14 multiparous women gave birth within 3 h after the last misoprostol dose.
Conclusions: In this historical cohort, three in ten women met the criteria for outpatient management of labor induction with oral misoprostol. Serious adverse events were rare. The average time span from the initiation of labor induction to the last misoprostol was nearly 24 h. This suggests a potential for low-risk women with an induced labor to spend a substantial period of time at home before labor onset. However, larger studies testing or evaluating labor induction with oral misoprostol as an outpatient procedure are needed to draw conclusions.
Keywords: birth; induction of labor; maternity care; misoprostol; obstetrics; outpatient labor induction.
© 2024 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
All authors confirm that there are no conflicts of interest.
Figures
Similar articles
-
Clinical outcomes and feasibility of implementing outpatient labor induction with misoprostol: A prospective cohort study.Acta Obstet Gynecol Scand. 2025 Apr;104(4):647-657. doi: 10.1111/aogs.15029. Epub 2025 Jan 29. Acta Obstet Gynecol Scand. 2025. PMID: 39878306 Free PMC article.
-
An audit of oral administration of Angusta® (misoprostol) 25 µg for induction of labor in 976 consecutive women with a singleton pregnancy in a university hospital in Denmark.Acta Obstet Gynecol Scand. 2020 Oct;99(10):1396-1402. doi: 10.1111/aogs.13876. Epub 2020 May 19. Acta Obstet Gynecol Scand. 2020. PMID: 32311758
-
Efficacy and safety of oral misoprostol vs transvaginal balloon catheter for labor induction: An observational study within the SWEdish Postterm Induction Study (SWEPIS).Acta Obstet Gynecol Scand. 2021 Aug;100(8):1463-1477. doi: 10.1111/aogs.14155. Epub 2021 May 2. Acta Obstet Gynecol Scand. 2021. PMID: 33768520 Clinical Trial.
-
Outpatient vs inpatient induction of labor with oral misoprostol: A retrospective study.Acta Obstet Gynecol Scand. 2023 May;102(5):605-611. doi: 10.1111/aogs.14550. Epub 2023 Mar 25. Acta Obstet Gynecol Scand. 2023. PMID: 36965000 Free PMC article.
-
Vaginal misoprostol administration for cervical ripening and labor induction.Clin Obstet Gynecol. 2006 Sep;49(3):627-41. doi: 10.1097/00003081-200609000-00021. Clin Obstet Gynecol. 2006. PMID: 16885668 Review.
Cited by
-
Clinical outcomes and feasibility of implementing outpatient labor induction with misoprostol: A prospective cohort study.Acta Obstet Gynecol Scand. 2025 Apr;104(4):647-657. doi: 10.1111/aogs.15029. Epub 2025 Jan 29. Acta Obstet Gynecol Scand. 2025. PMID: 39878306 Free PMC article.
References
-
- Simpson KR. Trends in labor induction in the United States, 1989 to 2020. MCN Am J Matern Child Nurs. 2022;47:235. - PubMed
-
- Medical Birth Registry of Norway. F8 Labor onset and labor induction [Internet]. 2022. Accessed June 2, 2023 https://statistikkbank.fhi.no/mfr/
-
- Coates R, Cupples G, Scamell A, McCourt C. Women's experiences of induction of labour: qualitative systematic review and thematic synthesis. Midwifery. 2019;69:17‐28. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
