

The role of the female gender on mid-term outcome after coronary artery bypass grafting: a retrospective study
- PMID: 38505022
- PMCID: PMC10944725
- DOI: 10.21037/jtd-23-932
The role of the female gender on mid-term outcome after coronary artery bypass grafting: a retrospective study
Abstract
Background: Data on female gender differences on clinical prognosis after coronary artery bypass grafting (CABG) are still controversial. We evaluated retrospectively the impact of women patients in comparison with men undergoing CABG on mid-term outcome.
Methods: Between December 2014 and March 2022, 1,044 consecutive patients (162 females, 15.5%, 882 males, 84.5%) underwent isolated CABG. The mean follow-up was 40±27 (median 38) months. Logistic and Cox model analysis regressions were used to assess the risk of female gender and other variables, Kaplan-Meier estimates to assess survival rates.
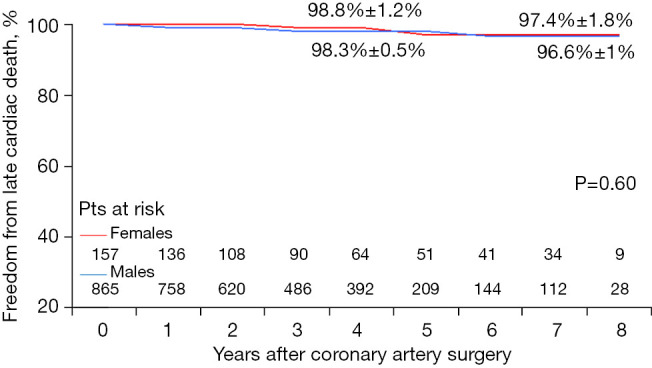
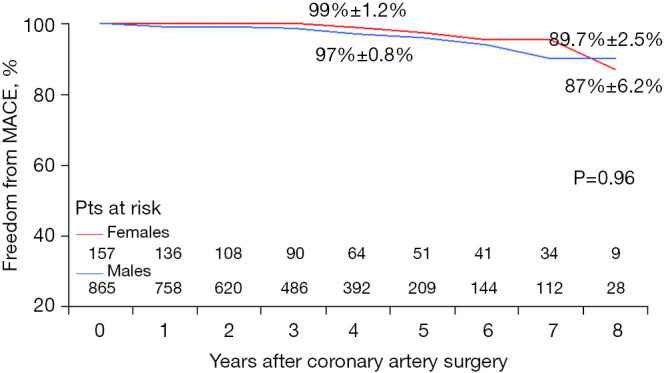
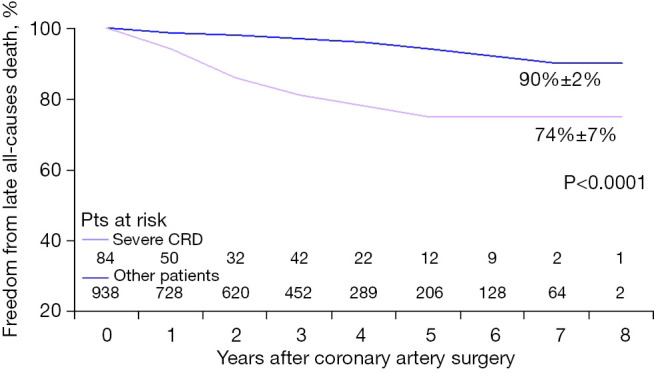
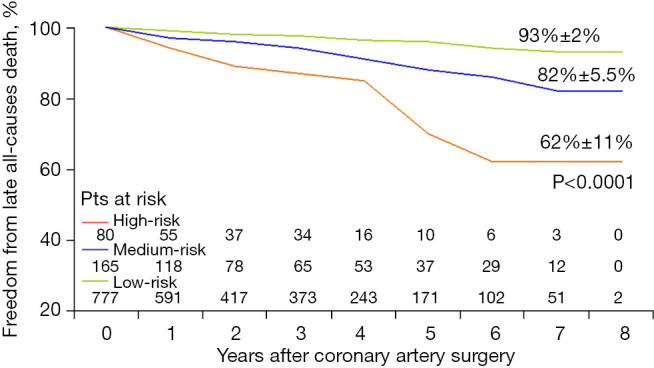
Results: Women did not have a significant higher operative mortality than men (3.09% vs. 1.93%; P=0.37). There was no difference in the use of left internal mammary artery (97.5% vs. 94.9%; P=0.85). Independent predictors of early mortality were emergency CABG (P<0.0001), percutaneous coronary intervention (PCI) within 30 days (P=0.0026), and higher EuroSCORE II (P=0.0155). At 7.5 years, actuarial survival was 87%±3.6% for female gender vs. 88%±1.9% in male gender (P=0.41), freedom from cardiac death 97%±1.8% vs. 96.6%±1.0% (P=0.6), freedom from major adverse cardiac events (MACE) 87%±6.2% vs. 89.7%±2.5% (P=0.96). Independent predictor of all-causes death and cardiac death was the advanced age (74 years in dead patients vs. 67 years in survivors) (P<0.0001). Female gender was not a predictor of either operative mortality (P=0.34) or worse mid-term outcome (P=0.41).
Conclusions: Women undergoing CABG with the same surgical techniques currently adopted for men, do not appear to be associated with worse early prognosis. Freedom from late all-causes mortality, cardiac death and adverse cardiac events are comparable and equally satisfactory, highlighting the positive protective effect of CABG over time also in women.
Keywords: Gender; coronary artery bypass grafting (CABG); women health.
2024 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-932/coif). The authors have no conflicts of interest to declare.
Figures

References
-
- Saxena A, Dinh D, Smith JA, et al. Sex differences in outcomes following isolated coronary artery bypass graft surgery in Australian patients: analysis of the Australasian Society of Cardiac and Thoracic Surgeons cardiac surgery database. Eur J Cardiothorac Surg 2012;41:755-62. 10.1093/ejcts/ezr039 - DOI - PubMed
-
- Lichtman JH, Leifheit EC, Safdar B, et al. Sex Differences in the Presentation and Perception of Symptoms Among Young Patients With Myocardial Infarction: Evidence from the VIRGO Study (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients). Circulation 2018;137:781-90. 10.1161/CIRCULATIONAHA.117.031650 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous