

Chylothorax: pathophysiology, diagnosis, and management-a comprehensive review
- PMID: 38505027
- PMCID: PMC10944732
- DOI: 10.21037/jtd-23-1636
Chylothorax: pathophysiology, diagnosis, and management-a comprehensive review
Abstract
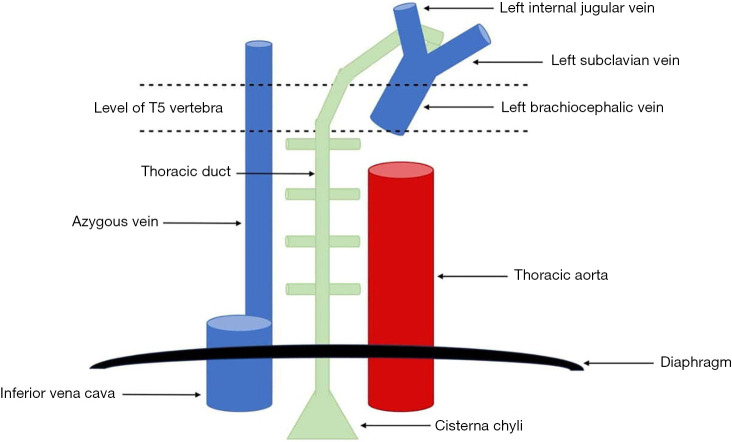
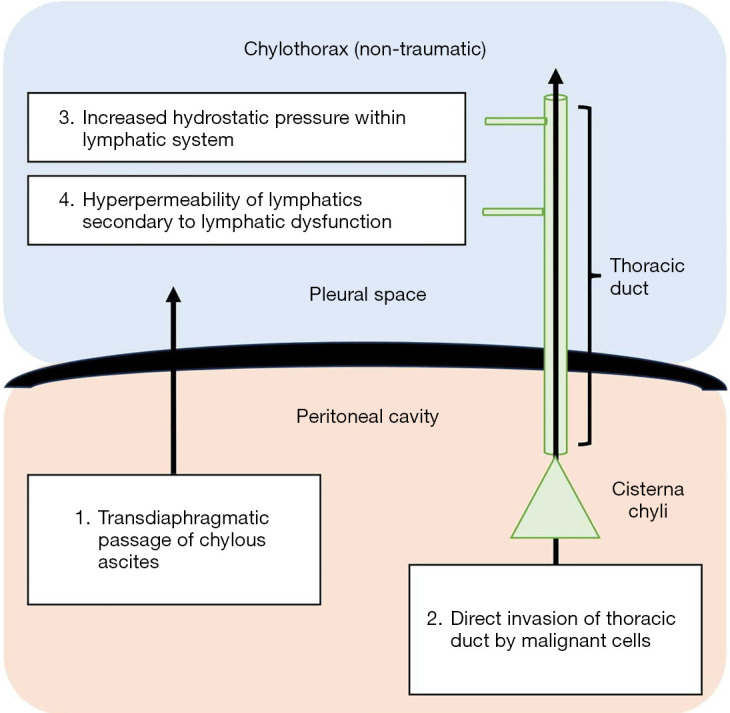
Chylothorax is a rare condition characterized by the accumulation of chyle in the pleural space. While it accounts for a small percentage of pleural effusions, chylothorax can lead to significant morbidity and mortality. This article provides a comprehensive overview of chylothorax, covering its relevant anatomy, aetiology, pathophysiology, clinical features, diagnosis, and management. Injury or disruption to the thoracic duct (which is responsible for chyle transport) leads to the development of chylothorax. This may result from trauma, such as iatrogenic injury during surgery, or non-traumatic causes, including malignancy, lymphatic disorders, and heart failure. Recognition of the underlying cause is essential to tailor management. Clinical presentation varies, with symptoms linked to rate of chyle accumulation and the causative condition. Diagnosis relies on pleural fluid analysis, with demonstration of elevated triglyceride levels (>110 mg/dL) and reduced cholesterol levels (<200 mg/dL) being the key diagnostic criteria employed in clinical practice. Various imaging modalities, including computed tomography (CT) scans and lymphatic-specific investigations, may be utilised to aid identification of the site of chyle leak, as well as determine the likely underlying cause. Chylothorax management is multifaceted, with conservative approaches such as dietary modification and pharmacological interventions often initiated as first-line treatment. Drainage of chylous effusion may be necessary for symptom relief. When conservative methods fail, interventional procedures like thoracic duct ligation or embolization can be considered. Due to the diverse aetiological factors and patient characteristics associated with chylothorax, individualized management strategies are recommended. Nonetheless, management of chylothorax is an evolving field with a paucity of high-quality evidence or standardized guidelines, highlighting the importance of ongoing research and a multidisciplinary approach to optimize individual patient care.
Keywords: Chylothorax; effusion; pleural disease.
2024 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-1636/coif). The series “Malignant and Benign Pleural Effusions” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures

References
-
- Sassoon CS, Light RW. Chylothorax and pseudochylothorax. Clin Chest Med 1985;6:163-71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources