

Alcohol Withdrawal Severity Measures for Identifying Patients Requiring High-Intensity Care
- PMID: 38505174
- PMCID: PMC10950191
- DOI: 10.1097/CCE.0000000000001066
Alcohol Withdrawal Severity Measures for Identifying Patients Requiring High-Intensity Care
Abstract
Objectives: Alcohol withdrawal syndrome (AWS) may progress to require high-intensity care. Approaches to identify hospitalized patients with AWS who received higher level of care have not been previously examined. This study aimed to examine the utility of Clinical Institute Withdrawal Assessment Alcohol Revised (CIWA-Ar) for alcohol scale scores and medication doses for alcohol withdrawal management in identifying patients who received high-intensity care.
Design: A multicenter observational cohort study of hospitalized adults with alcohol withdrawal.
Setting: University of Chicago Medical Center and University of Wisconsin Hospital.
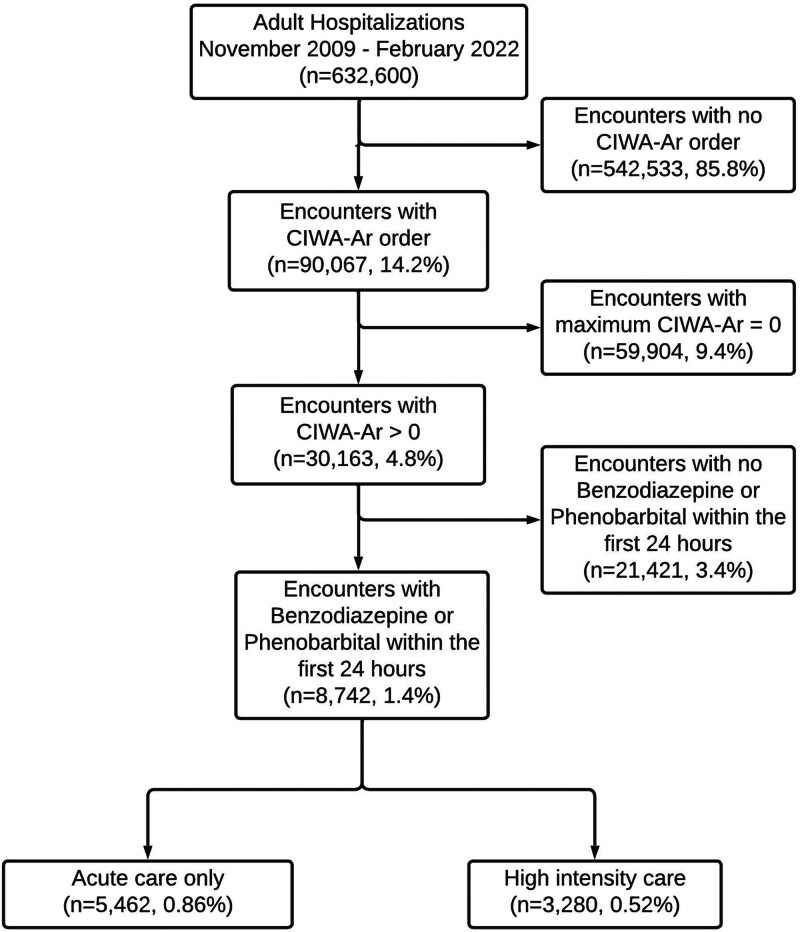
Patients: Inpatient encounters between November 2008 and February 2022 with a CIWA-Ar score greater than 0 and benzodiazepine or barbiturate administered within the first 24 hours. The primary composite outcome was patients who progressed to high-intensity care (intermediate care or ICU).
Interventions: None.
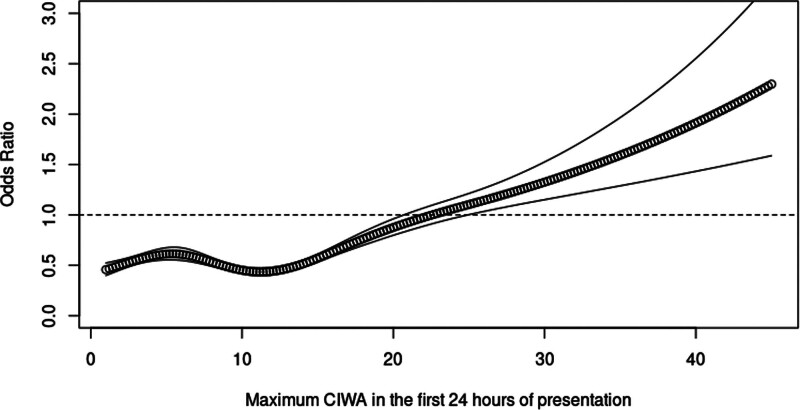
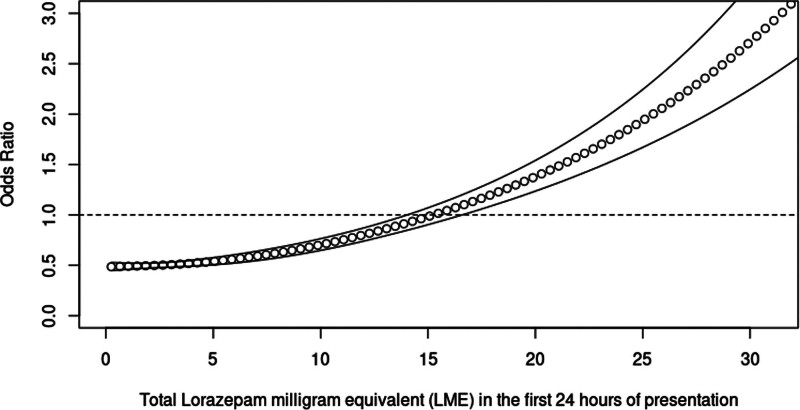
Main results: Among the 8742 patients included in the study, 37.5% (n = 3280) progressed to high-intensity care. The odds ratio for the composite outcome increased above 1.0 when the CIWA-Ar score was 24. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) at this threshold were 0.12 (95% CI, 0.11-0.13), 0.95 (95% CI, 0.94-0.95), 0.58 (95% CI, 0.54-0.61), and 0.64 (95% CI, 0.63-0.65), respectively. The OR increased above 1.0 at a 24-hour lorazepam milligram equivalent dose cutoff of 15 mg. The sensitivity, specificity, PPV, and NPV at this threshold were 0.16 (95% CI, 0.14-0.17), 0.96 (95% CI, 0.95-0.96), 0.68 (95% CI, 0.65-0.72), and 0.65 (95% CI, 0.64-0.66), respectively.
Conclusions: Neither CIWA-Ar scores nor medication dose cutoff points were effective measures for identifying patients with alcohol withdrawal who received high-intensity care. Research studies for examining outcomes in patients who deteriorate with AWS will require better methods for cohort identification.
Keywords: alcohol use disorder; benzodiazepines; inpatients; intensive care units; substance withdrawal syndrome.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Steel received funding from the National Institute on Alcohol Abuse and Alcoholism K23AA030588. Dr. Mayampurath received funding from the National Heart, Lung, and Blood Institute (NHLBI) K01HL148390. Dr. Matthew Churpek received funding from NHLBI R01HL157262. Dr. Afshar received funding from the National Institute on Drug Abuse R01DA051464. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Alvanzo A, Kleinschmidt K, Kmiec JA, et al. : The ASAM clinical practice guideline on alcohol withdrawal management. J Addict Med 2020; 14:1–72 - PubMed
-
- Nguyen TA, Lam SW: Phenobarbital and symptom-triggered lorazepam versus lorazepam alone for severe alcohol withdrawal in the intensive care unit. Alcohol 2020; 82:23–27 - PubMed
-
- Nisavic M, Nejad SH, Isenberg BM, et al. : Use of phenobarbital in alcohol withdrawal management—a retrospective comparison study of phenobarbital and benzodiazepines for acute alcohol withdrawal management in general medical patients. Psychosomatics 2019; 60:458–467 - PubMed
-
- Awissi D-K, Lebrun G, Fagnan M, et al. ; Regroupement de Soins Critiques, Réseau de Soins Respiratoires, Québec: Alcohol, nicotine, and iatrogenic withdrawals in the ICU. Crit Care Med 2013; 41:S57–S68 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
