

Development and internal validation of machine learning-based models and external validation of existing risk scores for outcome prediction in patients with ischaemic stroke
- PMID: 38505491
- PMCID: PMC10944684
- DOI: 10.1093/ehjdh/ztad073
Development and internal validation of machine learning-based models and external validation of existing risk scores for outcome prediction in patients with ischaemic stroke
Abstract
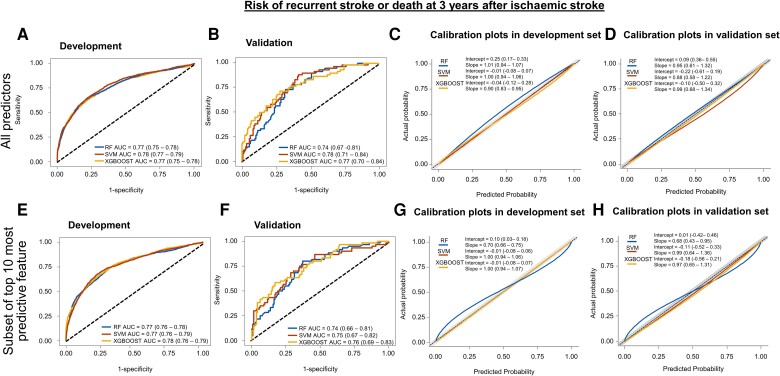
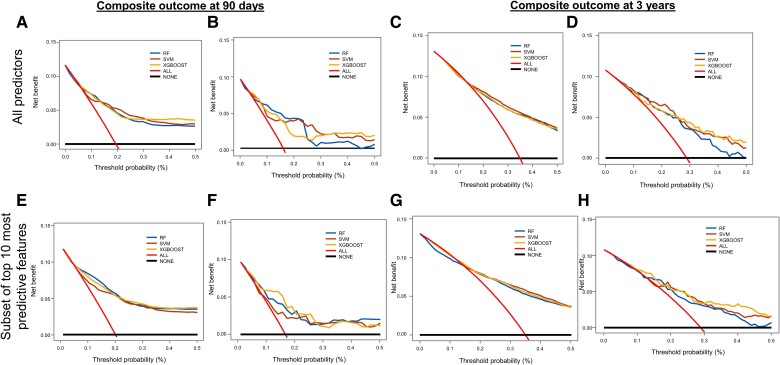
Aims: We developed new machine learning (ML) models and externally validated existing statistical models [ischaemic stroke predictive risk score (iScore) and totalled health risks in vascular events (THRIVE) scores] for predicting the composite of recurrent stroke or all-cause mortality at 90 days and at 3 years after hospitalization for first acute ischaemic stroke (AIS).
Methods and results: In adults hospitalized with AIS from January 2005 to November 2016, with follow-up until November 2019, we developed three ML models [random forest (RF), support vector machine (SVM), and extreme gradient boosting (XGBOOST)] and externally validated the iScore and THRIVE scores for predicting the composite outcomes after AIS hospitalization, using data from 721 patients and 90 potential predictor variables. At 90 days and 3 years, 11 and 34% of patients, respectively, reached the composite outcome. For the 90-day prediction, the area under the receiver operating characteristic curve (AUC) was 0.779 for RF, 0.771 for SVM, 0.772 for XGBOOST, 0.720 for iScore, and 0.664 for THRIVE. For 3-year prediction, the AUC was 0.743 for RF, 0.777 for SVM, 0.773 for XGBOOST, 0.710 for iScore, and 0.675 for THRIVE.
Conclusion: The study provided three ML-based predictive models that achieved good discrimination and clinical usefulness in outcome prediction after AIS and broadened the application of the iScore and THRIVE scoring system for long-term outcome prediction. Our findings warrant comparative analyses of ML and existing statistical method-based risk prediction tools for outcome prediction after AIS in new data sets.
Keywords: Machine-based learning; Mortality; Prediction models; Statistical; Stroke.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures




References
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation 2021;143:e254–e743. - PubMed
-
- Feng W, Hendry RM, Adams RJ. Risk of recurrent stroke, myocardial infarction, or death in hospitalized stroke patients. Neurology 2010;74:588–593. - PubMed
-
- Dhamoon MS, Sciacca RR, Rundek T, Sacco RL, Elkind MS. Recurrent stroke and cardiac risks after first ischemic stroke: the Northern Manhattan Study. Neurology 2006;66:641–646. - PubMed
-
- Hankey GJ, Jamrozik K, Broadhurst RJ, Forbes S, Burvill PW, Anderson CS, et al. Long-term risk of first recurrent stroke in the Perth Community Stroke Study. Stroke 1998;29:2491–2500. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources