

Morbidity After Mechanical Bowel Preparation and Oral Antibiotics Prior to Rectal Resection: The MOBILE2 Randomized Clinical Trial
- PMID: 38506889
- PMCID: PMC10955353
- DOI: 10.1001/jamasurg.2024.0184
Morbidity After Mechanical Bowel Preparation and Oral Antibiotics Prior to Rectal Resection: The MOBILE2 Randomized Clinical Trial
Erratum in
-
Error in the Visual Abstract.JAMA Surg. 2024 Jun 1;159(6):722. doi: 10.1001/jamasurg.2024.1123. JAMA Surg. 2024. PMID: 38656330 Free PMC article. No abstract available.
Abstract
Importance: Surgical site infections (SSIs)-especially anastomotic dehiscence-are major contributors to morbidity and mortality after rectal resection. The role of mechanical and oral antibiotics bowel preparation (MOABP) in preventing complications of rectal resection is currently disputed.
Objective: To assess whether MOABP reduces overall complications and SSIs after elective rectal resection compared with mechanical bowel preparation (MBP) plus placebo.
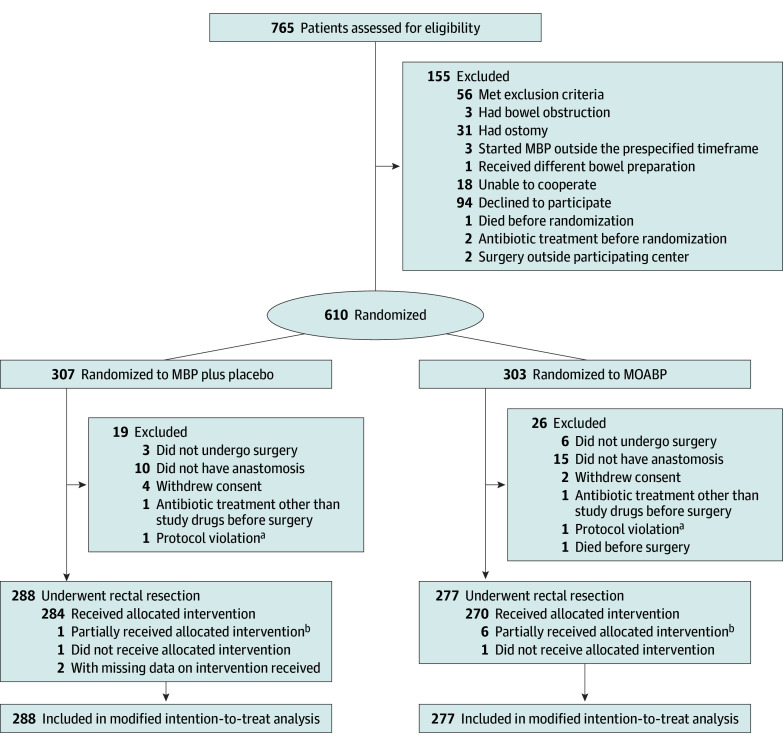
Design, setting, and participants: This multicenter, double-blind, placebo-controlled randomized clinical trial was conducted at 3 university hospitals in Finland between March 18, 2020, and October 10, 2022. Patients aged 18 years and older undergoing elective resection with primary anastomosis of a rectal tumor 15 cm or less from the anal verge on magnetic resonance imaging were eligible for inclusion. Outcomes were analyzed using a modified intention-to-treat principle, which included all patients who were randomly allocated to and underwent elective rectal resection with an anastomosis.
Interventions: Patients were stratified according to tumor distance from the anal verge and neoadjuvant treatment given and randomized in a 1:1 ratio to receive MOABP with an oral regimen of neomycin and metronidazole (n = 277) or MBP plus matching placebo tablets (n = 288). All study medications were taken the day before surgery, and all patients received intravenous antibiotics approximately 30 minutes before surgery.
Main outcomes and measures: The primary outcome was overall cumulative postoperative complications measured using the Comprehensive Complication Index. Key secondary outcomes were SSI and anastomotic dehiscence within 30 days after surgery.
Results: In all, 565 patients were included in the analysis, with 288 in the MBP plus placebo group (median [IQR] age, 69 [62-74] years; 190 males [66.0%]) and 277 in the MOABP group (median [IQR] age, 70 [62-75] years; 158 males [57.0%]). Patients in the MOABP group experienced fewer overall postoperative complications (median [IQR] Comprehensive Complication Index, 0 [0-8.66] vs 8.66 [0-20.92]; Wilcoxon effect size, 0.146; P < .001), fewer SSIs (23 patients [8.3%] vs 48 patients [16.7%]; odds ratio, 0.45 [95% CI, 0.27-0.77]), and fewer anastomotic dehiscences (16 patients [5.8%] vs 39 patients [13.5%]; odds ratio, 0.39 [95% CI, 0.21-0.72]) compared with patients in the MBP plus placebo group.
Conclusions and relevance: Findings of this randomized clinical trial indicate that MOABP reduced overall postoperative complications as well as rates of SSIs and anastomotic dehiscences in patients undergoing elective rectal resection compared with MBP plus placebo. Based on these findings, MOABP should be considered as standard treatment in patients undergoing elective rectal resection.
Trial registration: ClinicalTrials.gov Identifier: NCT04281667.
Conflict of interest statement
Figures
Comment in
-
Mechanical and Oral Antibiotic Bowel Preparation in Elective Rectal Resection.JAMA Surg. 2024 Jun 1;159(6):615. doi: 10.1001/jamasurg.2024.0174. JAMA Surg. 2024. PMID: 38506855 No abstract available.
References
-
- World Health Organization . Global guidelines for the prevention of surgical site infection. 2nd ed. World Health Organization. 2018. Accessed May 30, 2023. https://apps.who.int/iris/handle/10665/277399
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
