

Evaluation of vital signs through a mobile application in patients with heart failure: a opportunity for remote titration?
- PMID: 38507315
- PMCID: PMC11160516
- DOI: 10.24875/ACM.22000221
Evaluation of vital signs through a mobile application in patients with heart failure: a opportunity for remote titration?
Abstract
Background: Virtual consultations have increased exponentially, but a limitation is the inability to assess vital signs (VS). This is particularly useful in patients with heart failure (HF) for titrating prognosis-modifying medication. This issue could potentially be addressed by a tool capable of measuring blood pressure (BP) and heart rate (HR) accurately, remotely, and conveniently. Mobile phones equipped with transdermal optical imaging technology could meet these requirements.
Objective: To evaluate the accuracy of a transdermal optical imaging-based app for estimating VS compared to clinical assessment in patients with HF.
Methods: A prospective cohort study included patients evaluated in an HF outpatient unit between February and April 2022. BP and HR were simultaneously assessed using the app and clinical examination (BP with an automated sphygmomanometer and HR by brachial palpation). Three measurements were taken by both the app and clinic for each patient, by two independent blinded physicians.
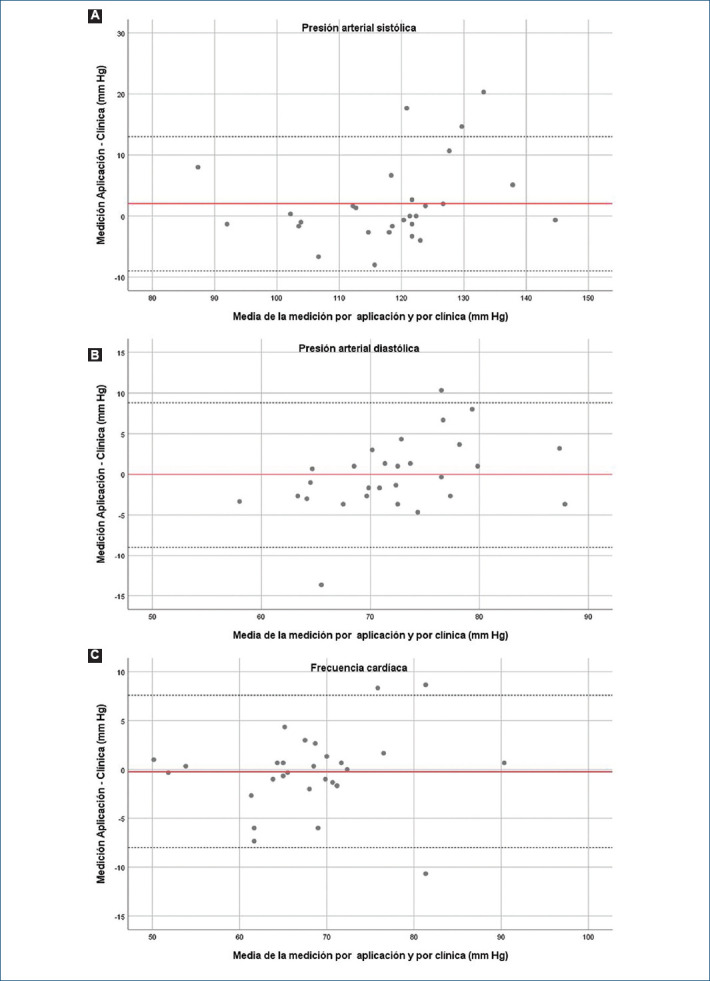
Results: Thirty patients were included, with 540 measurements of BP and HR. The mean age was 66 (± 13) years, 53.3% were male. The mean left ventricular ejection fraction was 37 ± 15, with 63.3% having previous hospitalizations for HF, and 63.4% in NYHA class II-III. The mean difference between the app measurement and its clinical reference measurement was 3.6 ± 0.5 mmHg for systolic BP (SBP), 0.9 ± -0.2 mmHg for diastolic BP (DBP), and 0.2 ± 0.4 bpm for HR. When averaging the paired mean differences for each patient, the mean across the 30 patients was 2 ± 6 mmHg for SBP, -0.14 ± 4.6 mmHg for DBP, and 0.23 ± 4 bpm for HR.
Conclusion: The estimation of BP and HR by an app with transdermal optical imaging technology was comparable to non-invasive measurement in patients with HF and met the precision criteria for BP measurement in this preliminary study. The use of this new transdermal optical imaging technology provides promising data, which should be corroborated in larger cohorts.
Antecedentes: Las consultas virtuales aumentaron exponencialmente, pero presentan como limitación la imposibilidad de valorar los signos vitales (SV), siendo especialmente útiles en los pacientes con insuficiencia cardiaca (IC) para titular medicación que modifica pronóstico. Este problema podría potencialmente solucionarse mediante una herramienta que pueda medir la presión arterial (PA) y frecuencia cardiaca (FC) de manera precisa, accesible y remota. Los teléfonos móviles equipados con tecnología de imágenes ópticas transdérmicas podrían cumplir con estos requisitos.
Objetivo: Evaluar la precisión de una app basada en imagen óptica transdérmica para estimar SV en relación con la valoración clínica en pacientes con IC.
Métodos: Estudio de cohorte prospectivo, se incluyeron pacientes evaluados en una unidad ambulatoria de IC de febrero a abril del 2022. Se valoró simultáneamente la PA y FC mediante la app y el examen clínico (PA con un esfigmomanómetro automatizado y FC por palpación braquial). Se realizaron tres mediciones por app y clínica en cada paciente, por dos médicos independientes, encontrándose ciegos a los resultados.
Resultados: Se incluyeron 30 pacientes, con 540 mediciones de TA y de FC. Edad media de 66 (± 13) años, el 53.3% de sexo masculino. La fracción de eyección del ventrículo izquierdo media fue de 37 ± 15, con hospitalizaciones previas por IC el 63.3%, en CF II-III el 63.4%. La diferencia media entre la medición de la app y su medición de referencia clínica fue de 3.6 ± 0.5 mmHg para PA sistólica (PAS), 0.9 ± –0.2 mmHg para PA diastólica (PAD) y 0.2 ± 0.4 lpm para FC. Cuando se promedian las diferencias medias emparejadas para cada paciente, la media entre los 30 pacientes es de 2 ± 6 mmHg para PAS, –0.14 ± 4.6 mmHg para PAD y 0.23 ± 4 lpm para FC.
Conclusión: La estimación de PA y FC por una app con tecnología de imagen óptica transdérmica fue comparable a la medición no invasiva en pacientes con IC, y cumple los criterios de precisión de la medición de PA en este estudio preliminar. La utilización de esta nueva tecnología de imagen óptica transdérmica brinda datos prometedores, que deberán ser corroborados en cohortes de mayor tamaño.
Keywords: Aplicación móvil; Artificial intelligence; Heart failure; Insuficiencia cardíaca; Inteligencia artificial; Mobile application; Signos vitales; Smartphone; Teléfono inteligente; Vital signs.
Copyright: © 2024 Permanyer.
Conflict of interest statement
Ninguno.
Figures


References
-
- van Riet EE, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH. Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail. 2016;18:242–52. - PubMed
-
- McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, et al. ESC Guidelines for the diagnosis and treatment of acute chronic heart failure 2012. Eur Heart J. 2012;33:1787–847. - PubMed
-
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol. 2013;61:391–403. - PubMed
-
- Berkowitz R, Blank LJ, Powell SK. Strategies to reduce hospitalization in the management of heart failure. Lippincotts Case Manag. 2005;10(6 Suppl):S1–S17. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous