

Comparison of Contemporary Risk Scores in All Groups of Pulmonary Hypertension: A Pulmonary Vascular Research Institute GoDeep Meta-Registry Analysis
- PMID: 38508334
- PMCID: PMC11443244
- DOI: 10.1016/j.chest.2024.03.018
Comparison of Contemporary Risk Scores in All Groups of Pulmonary Hypertension: A Pulmonary Vascular Research Institute GoDeep Meta-Registry Analysis
Abstract
Background: Pulmonary hypertension (PH) is a heterogeneous disease with a poor prognosis. Accurate risk stratification is essential for guiding treatment decisions in pulmonary arterial hypertension (PAH). Although various risk models have been developed for PAH, their comparative prognostic potential requires further exploration. Additionally, the applicability of risk scores in PH groups beyond group 1 remains to be investigated.
Research question: Are risk scores originally developed for PAH predictive in PH groups 1 through 4?
Study design and methods: We conducted a comprehensive analysis of outcomes among patients with incident PH enrolled in the multicenter worldwide Pulmonary Vascular Research Institute GoDeep meta-registry. Analyses were performed across PH groups 1 through 4 and further subgroups to evaluate the predictive value of PAH risk scores, including the Registry to Evaluate Early and Long-Term PAH Disease Mangement (REVEAL) Lite 2, REVEAL 2.0, European Society of Cardiology/European Respiratory Society 2022, Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA) 3-strata, and COMPERA 4-strata.
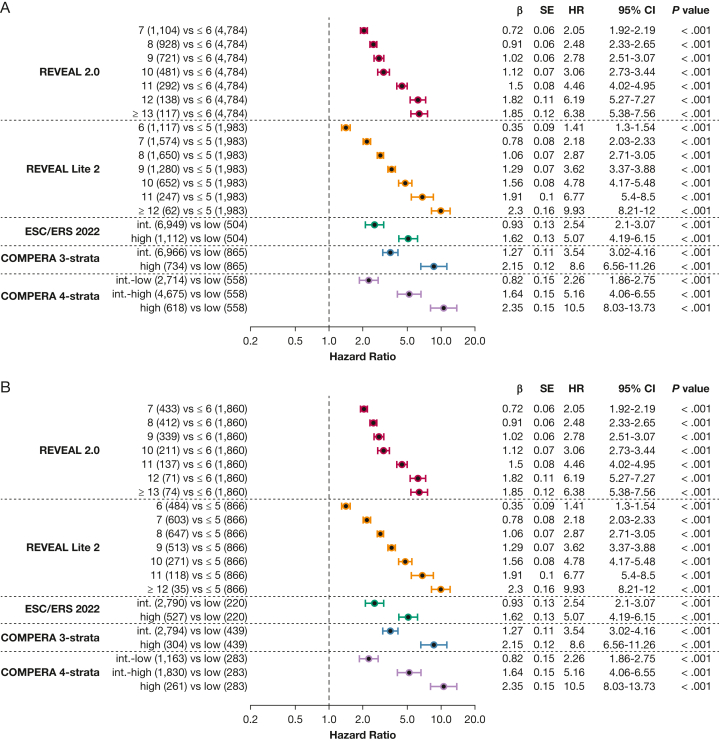
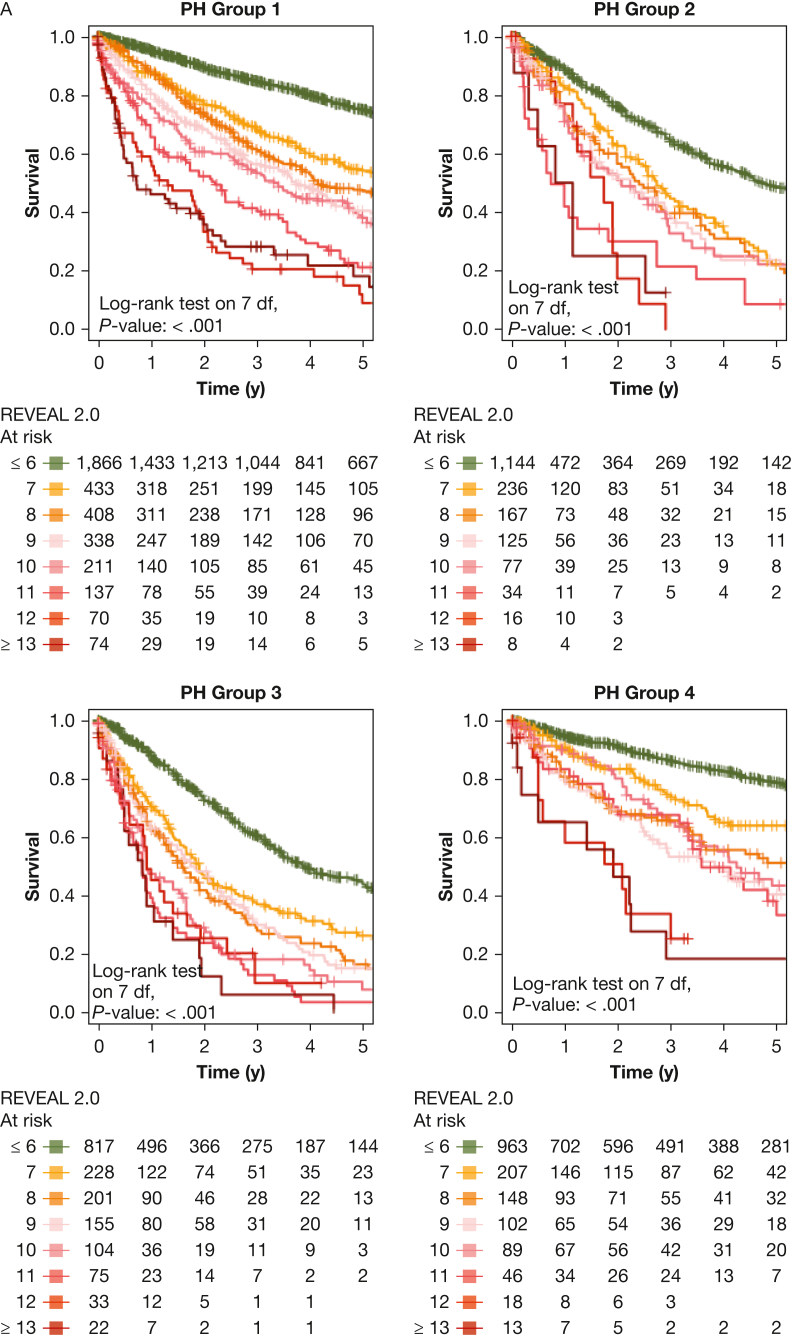
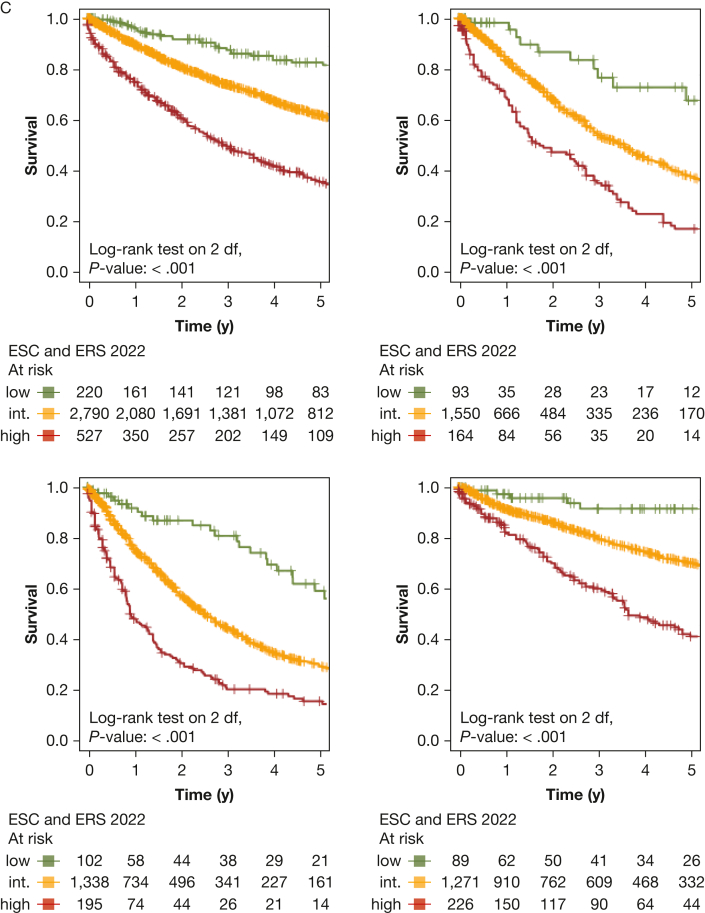
Results: Eight thousand five hundred sixty-five patients were included in the study, of whom 3,537 patients were assigned to group 1 PH, whereas 1,807 patients, 1,635 patients, and 1,586 patients were assigned to group 2 PH, group 3 PH, and group 4 PH, respectively. Pulmonary hemodynamics were impaired with median mean pulmonary arterial pressure of 42 mm Hg (interquartile range, 33-52 mm Hg) and pulmonary vascular resistance of 7 Wood units (WU) (interquartile range, 4-11 WU). All risk scores were prognostic in the entire PH population and in each of the PH groups 1 through 4. The REVEAL scores, when used as continuous prediction models, demonstrated the highest statistical prognostic power and granularity; the COMPERA 4-strata risk score provided subdifferentiation of the intermediate-risk group. Similar results were obtained when separately analyzing various subgroups (PH subgroups 1.1, 1.4.1, and 1.4.4; PH subgroups 3.1 and 3.2; group 2 with isolated postcapillary PH vs combined precapillary and postcapillary PH; patients of all groups with concomitant cardiac comorbidities; and severe [> 5 WU] vs nonsevere PH).
Interpretation: This comprehensive study with real-world data from 15 PH centers showed that PAH-designed risk scores possess predictive power in a large PH cohort, whether considered as common to the group or calculated separately for each PH group (1-4) and various subgroups.
Trial registry: ClinicalTrials.gov; No.: NCT05329714; URL: www.
Clinicaltrials: gov.
Keywords: PVRI GoDeep meta-registry; multicenter; predictive power; pulmonary hypertension; risk stratification.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial/Nonfinancial Disclosures The authors have reported to CHEST the following: A. Y. has received personal fees from MSD. H. G. has received personal fees from Actelion, AstraZeneca, Bayer, BMS, GossamerBio, GSK, Janssen-Cilag, Lilly, MSD, Novartis, OMT, Pfizer, and United Therapeutics. M. R. W. reports personal fees from MorphogenIX, Janssen, Chiesi, and Aerami; grants from British Heart Foundation and NIHR; and personal fees from MSD, Benevolent AI, and Tiakis Biotech, outside the submitted work. L. H. reports personal fees and nonfinancial support from Janssen and personal fees from MSD, Gossamer, and Altavant. D. G. K. reports support for the present manuscript from the Sheffield Biomedical Research Centre and consulting fees and other payments from Jansen Pharmaceuticals, Ferrer, Altavant, MSD, and United therapeutics. P. M. H. reports personal fees from Merck Co. S. Y. C. reports personal fees from Janssen, Bayer, Pfizer, United Therapeutics, and Acceleron Pharma and is a director, officer, and shareholder of Synhale Therapeutics. S. O. reports personal fees from MSD, Janssen, and Gallenica-Ferrer. H. A. G. has received fees from Actelion, AstraZeneca, Bayer, GSK, Janssen-Cilag, Lilly, Novartis, OMT, Pfizer, and United Therapeutics. M. J. R. has received support from Janssen Pharmaceutica and Bayer Pharma AG and speaker fees from Janssen Pharmaceutica and OMT. S. S. reports personal fees from Gossamer Bio, Merck, Keros, Janssen, United Therapeutics, and Liquidia. K. T. has received personal fees from Bayer, AstraZeneca, and Gossamer. W. S. has received consultancy fees from United Therapeutics, Tiakis Biotech AG, Liquidia, Pieris Pharmaceuticals, Abivax, Pfitzer, and Medspray BV. None declared (M. Fünderich, A.L., Y. S., O. T., A. J. S., R. T. Z., P. G. W., M. Frauendorf, A. Arvanitaki, G. G., K. S., H. R. C., R. F., I. A. G., E. B., J. S. A., A. P., S. G., A. Anthi, R. W. M., J. W., F. G.)
Figures








References
-
- Humbert M., Kovacs G., Hoeper M.M., et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43(38):3618–3731. - PubMed
-
- Gall H., Felix J.F., Schneck F.K., et al. The Giessen Pulmonary Hypertension Registry: survival in pulmonary hypertension subgroups. J Heart Lung Transplant. 2017;36(9):957–967. - PubMed
-
- Douschan P., Kovacs G., Avian A., et al. Mild elevation of pulmonary arterial pressure as a predictor of mortality. Am J Respir Crit Care Med. 2018;197(4):509–516. - PubMed
-
- Kovacs G., Berghold A., Scheidl S., Olschewski H. Pulmonary arterial pressure during rest and exercise in healthy subjects: a systematic review. Eur Respir J. 2009;34(4):888–894. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
