

A New Method to Predict Postoperative Stem Anteversion in Total Hip Arthroplasty for Developmental Dysplasia of the Hip
- PMID: 38509013
- PMCID: PMC11062849
- DOI: 10.1111/os.14037
A New Method to Predict Postoperative Stem Anteversion in Total Hip Arthroplasty for Developmental Dysplasia of the Hip
Abstract
Background: Preoperative evaluation of femoral anteversion to predict postoperative stem anteversion aids the selection of an appropriate prosthesis and optimizes the combined anteversion in total hip arthroplasty (THA) for developmental dysplasia of the hip (DDH). The conventional prediction methods are based on the femoral anteversion measurement at the location of the femoral head and/or neck. However, varied differences between femoral anteversion and postoperative stem anteversion were demonstrated. This study investigated the predictive role of a new method based on the principle of sagittal three-point fixation.
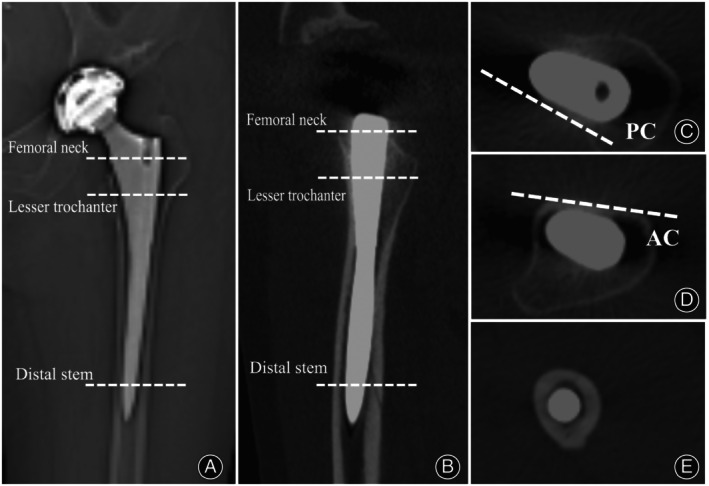
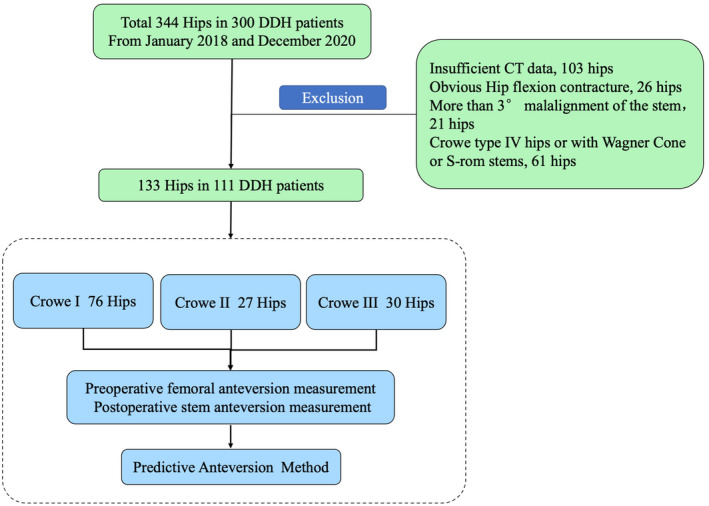
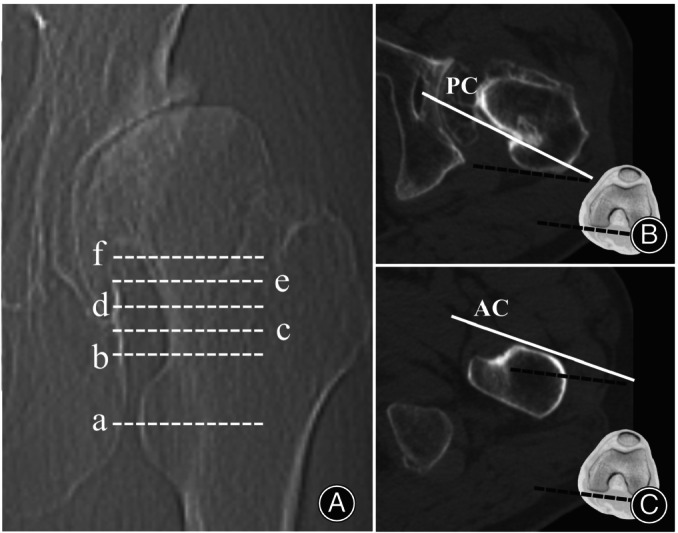
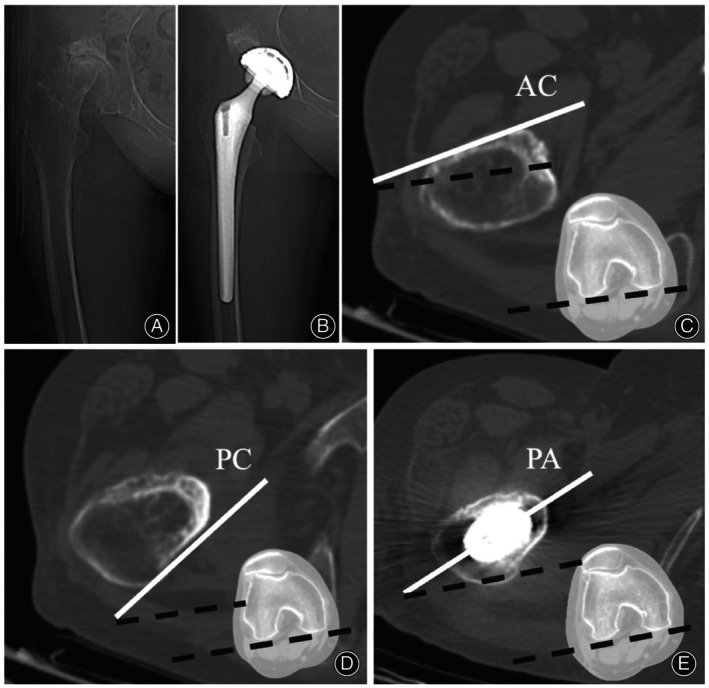
Methods: From January 2017 to December 2018, a total of 133 DDH hips that underwent THA were retrospectively analyzed. There were 76 Crowe type I, 27 type II, and 30 type III hips. The single-wedge stem was used in 49 hips, and the double-wedge stem was used in 84 hips. Preoperative native femoral anteversion at the femoral head-neck junction, anterior cortex anteversion at 2 levels of the lesser trochanter, posterior cortex anteversion at 5 levels of the femoral neck, and postoperative stem anteversion were measured using two-dimensional computed tomography. Predictive anteversion by the new method was calculated as the average anteversion formed by the anterior cortex at the lesser trochanter and the posterior cortex at the femoral neck.
Results: For hips with different neck heights, different Crowe types, different stem types, or different femoral anteversions, native femoral anteversion showed widely varied differences and correlations with stem anteversion, with differences ranging from -1.27 ± 8.33° to -13.67 ± 9.47° and correlations ranging from 0.122 (p = 0.705, no correlation) to 0.813. Predictive anteversion formed by the anterior cortex at the lesser trochanter proximal base and posterior cortex 10 mm above the lesser trochanter proximal base showed no significant difference with stem anteversion, with less varied differences (0.92 ± 7.52°) and good to excellent correlations (r = 0.826).
Conclusion: Adopting our new method, predictive anteversion, measured as the average anteversion of the anterior cortex at the lesser trochanter proximal base and posterior cortex 10 mm above the lesser trochanter proximal base, predicted postoperative stem anteversion more reliably than native femoral anteversion.
Keywords: Developmental Dysplasia of the Hip; Femoral Anteversion; Stem Anteversion; Total Hip Arthroplasty.
© 2024 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Prediction of Postoperative Stem Anteversion in Crowe Type II/III Developmental Dysplasia of the Hip on Preoperative Two-Dimensional Computed Tomography.J Arthroplasty. 2020 Feb;35(2):457-464. doi: 10.1016/j.arth.2019.09.037. Epub 2019 Sep 26. J Arthroplasty. 2020. PMID: 31668697
-
Optimal Level of Femoral Neck for Predicting Postoperative Stem Anteversion in Total Hip Arthroplasty for Crowe Type I Dysplastic Hip.Orthop Surg. 2020 Apr;12(2):480-487. doi: 10.1111/os.12647. Epub 2020 Mar 22. Orthop Surg. 2020. PMID: 32202054 Free PMC article.
-
The Effect of the Morphology of the Femur and Acetabulum in Dysplastic Hips on the Selection of Arthroplasty Femoral Implants: A Computer Tomography-Based Study.Orthop Surg. 2024 Nov;16(11):2793-2802. doi: 10.1111/os.14213. Epub 2024 Aug 28. Orthop Surg. 2024. PMID: 39198975 Free PMC article.
-
[Three-dimensional morphological study of the effect of false acetabulum on the femoral structure in Crowe type Ⅳ developmental dysplasia of the hip].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022 Jun 15;36(6):714-721. doi: 10.7507/1002-1892.202202016. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022. PMID: 35712929 Free PMC article. Chinese.
-
[Advances in revision surgery after primary total hip arthroplasty for Crowe type Ⅳ developmental dysplasia of the hip].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 Dec 15;37(12):1548-1555. doi: 10.7507/1002-1892.202309016. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 38130200 Free PMC article. Review. Chinese.
References
-
- Ferguson RJ, Palmer AJR, Taylor A, Porter ML, Malchau H, Glyn‐Jones S. Hip replacement. Lancet. 2018;392:1662–1671. - PubMed
-
- Greber EM, Pelt CE, Gililland JM, Anderson MB, Erickson JA, Peters CL. Challenges in total hip arthroplasty in the setting of developmental dysplasia of the hip. J Arthroplasty. 2017;32:S38–S44. - PubMed
-
- Perry KI, Berry DJ. Femoral considerations for total hip replacement in hip dysplasia. Orthop Clin North Am. 2012;43:377–386. - PubMed
-
- Zhang J, Wang L, Mao Y, Li H, Ding H, Zhu Z. The use of combined anteversion in total hip arthroplasty for patients with developmental dysplasia of the hip. J Arthroplasty. 2014;29:621–625. - PubMed
-
- Dorr LD, Zhinian W, Aamer M, Jinjun Z, Manish D, Prashant D. A comparison of surgeon estimation and computed tomographic measurement of femoral component anteversion in cementless total hip arthroplasty. J Bone Joint Surg Am. 2009;91:2598–2604. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
