

Functional Validation of Doxorubicin-Induced Cardiotoxicity-Related Genes
- PMID: 38510289
- PMCID: PMC10950437
- DOI: 10.1016/j.jaccao.2023.11.008
Functional Validation of Doxorubicin-Induced Cardiotoxicity-Related Genes
Abstract
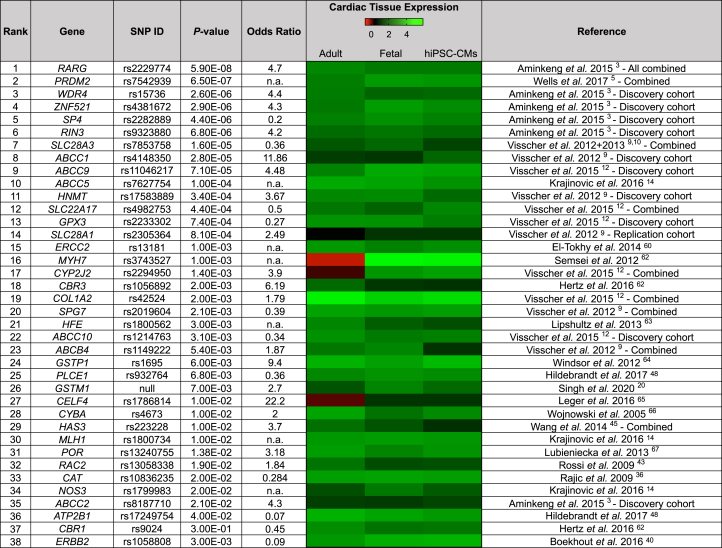
Background: Genome-wide association studies and candidate gene association studies have identified more than 180 genetic variants statistically associated with anthracycline-induced cardiotoxicity (AIC). However, the lack of functional validation has hindered the clinical translation of these findings.
Objectives: The aim of this study was to functionally validate all genes associated with AIC using human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs).
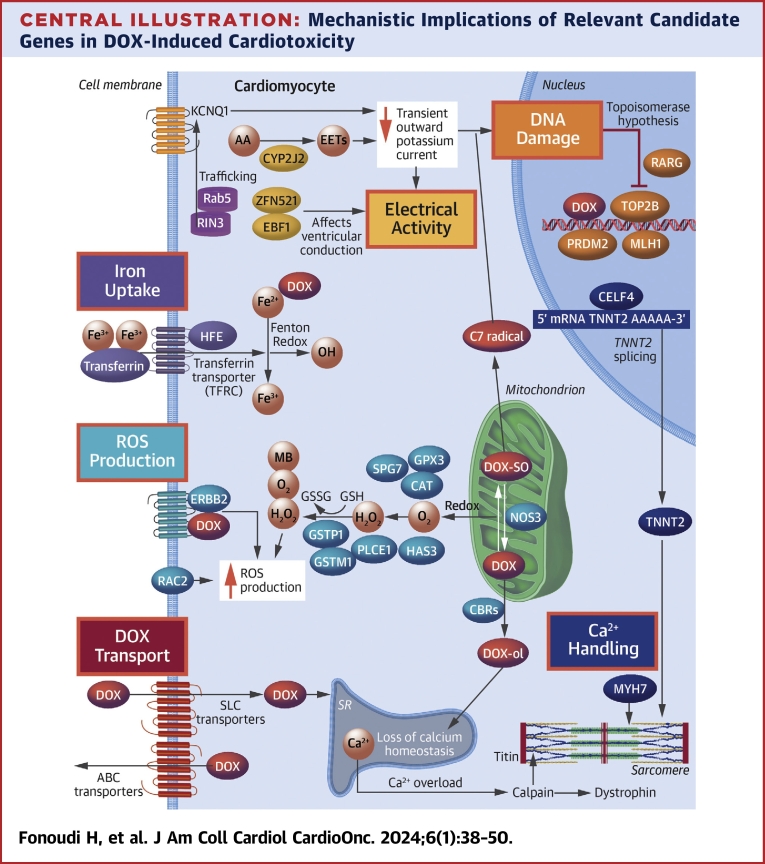
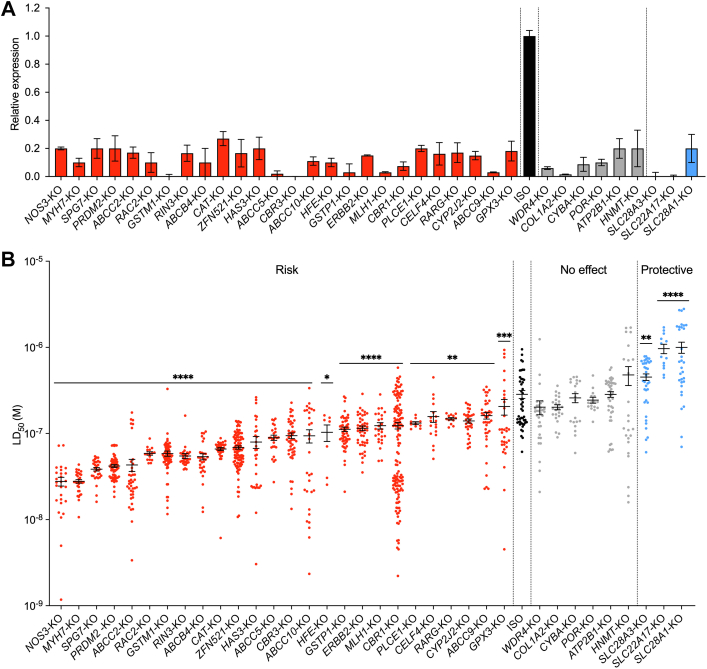
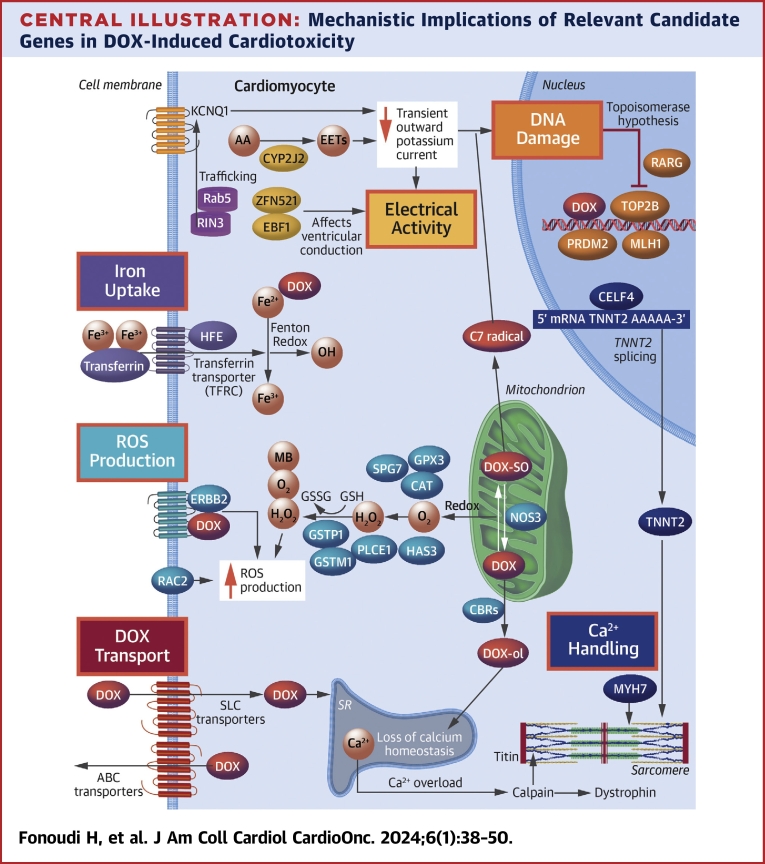
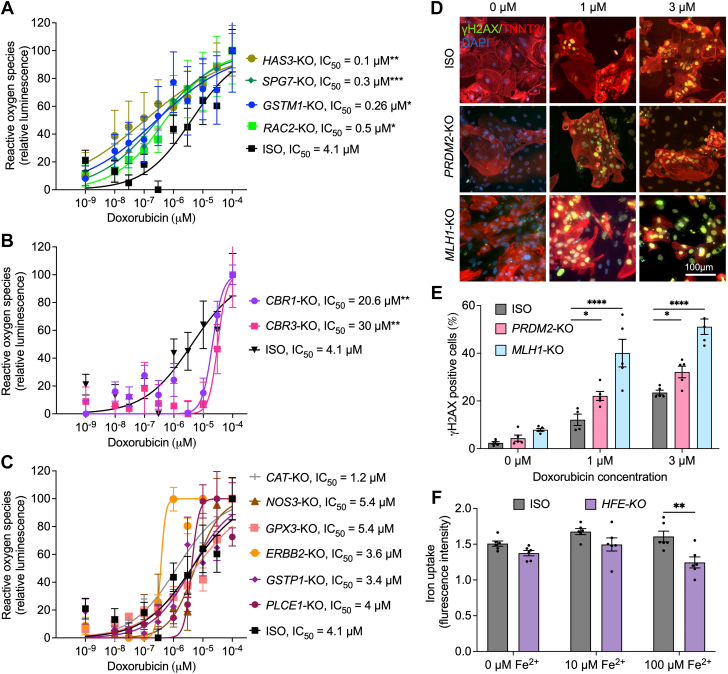
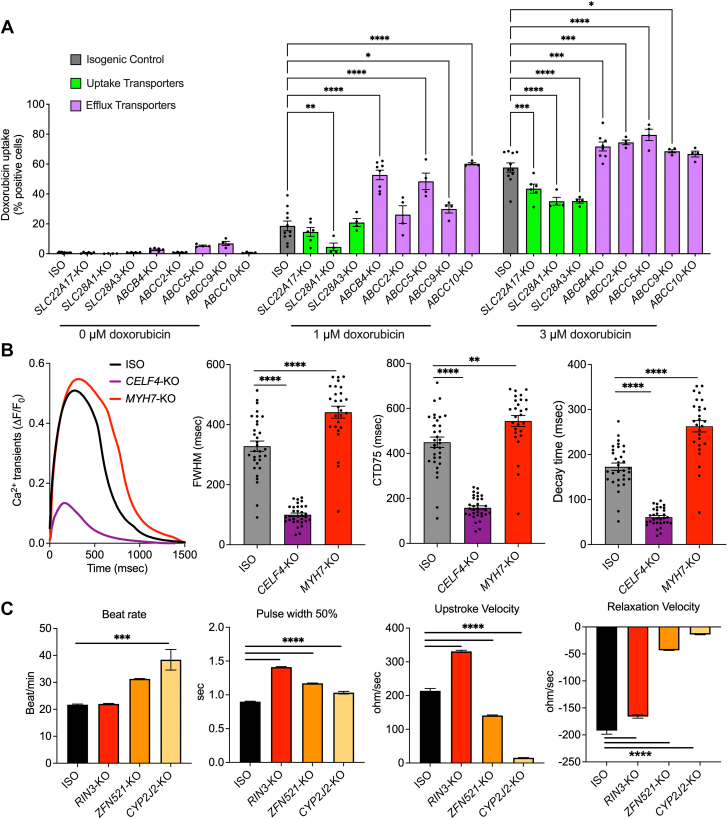
Methods: Through a systemic literature search, 80 genes containing variants significantly associated with AIC were identified. Additionally, 3 more genes with potential roles in AIC (GSTM1, CBR1, and ERBB2) were included. Of these, 38 genes exhibited expression in human fetal heart, adult heart, and hiPSC-CMs. Using clustered regularly interspaced short palindromic repeats/Cas9-based genome editing, each of these 38 genes was systematically knocked out in control hiPSC-CMs, and the resulting doxorubicin-induced cardiotoxicity (DIC) phenotype was assessed using hiPSC-CMs. Subsequently, functional assays were conducted for each gene knockout on the basis of hypothesized mechanistic implications in DIC.
Results: Knockout of 26 genes increased the susceptibility of hiPSC-CMs to DIC. Notable genes included efflux transporters (ABCC10, ABCC2, ABCB4, ABCC5, and ABCC9), well-established DIC-associated genes (CBR1, CBR3, and RAC2), and genome-wide association study-discovered genes (RARG and CELF4). Conversely, knockout of ATP2B1, HNMT, POR, CYBA, WDR4, and COL1A2 had no significant effect on the in vitro DIC phenotype of hiPSC-CMs. Furthermore, knockout of the uptake transporters (SLC28A3, SLC22A17, and SLC28A1) demonstrated a protective effect against DIC.
Conclusions: The present findings establish a comprehensive platform for the functional validation of DIC-associated genes, providing insights for future studies in DIC variant associations and potential mechanistic targets for the development of cardioprotective drugs.
Keywords: GWAS; cardiomyocytes; doxorubicin; genomics; human induced pluripotent stem cells.
© 2024 The Authors.
Conflict of interest statement
This work was supported by National Institutes of Health grants R01 CA220002 and R01 CA261898, American Heart Association Transformational Project Award 18TPA34230105, and the Leducq Foundation (to Dr Burridge). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
