

Caloric Restriction Rejuvenates Skeletal Muscle Growth in Heart Failure With Preserved Ejection Fraction
- PMID: 38510717
- PMCID: PMC10950401
- DOI: 10.1016/j.jacbts.2023.09.014
Caloric Restriction Rejuvenates Skeletal Muscle Growth in Heart Failure With Preserved Ejection Fraction
Abstract
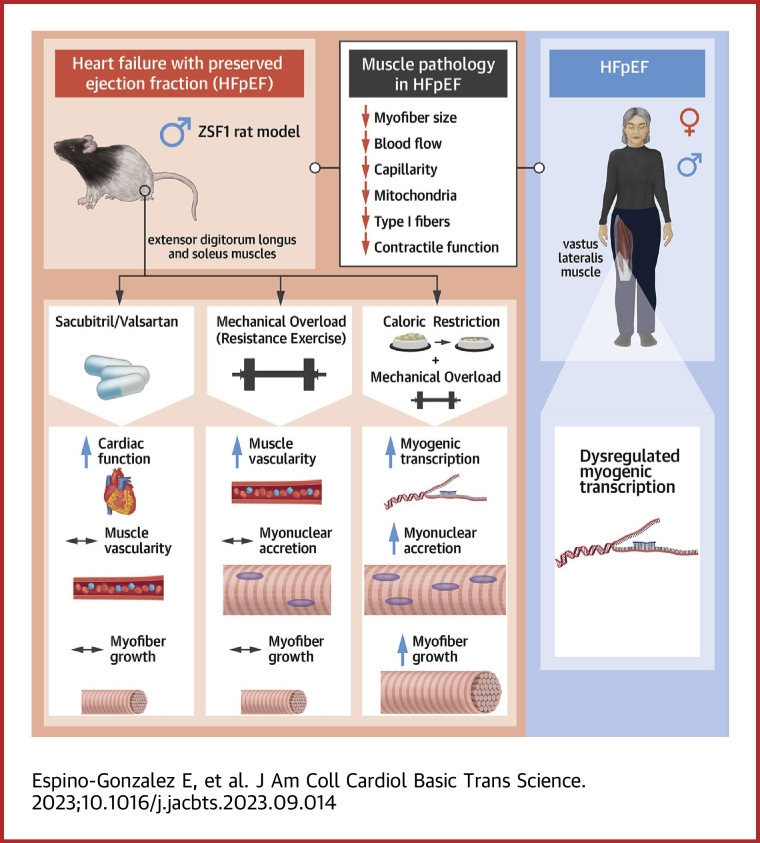
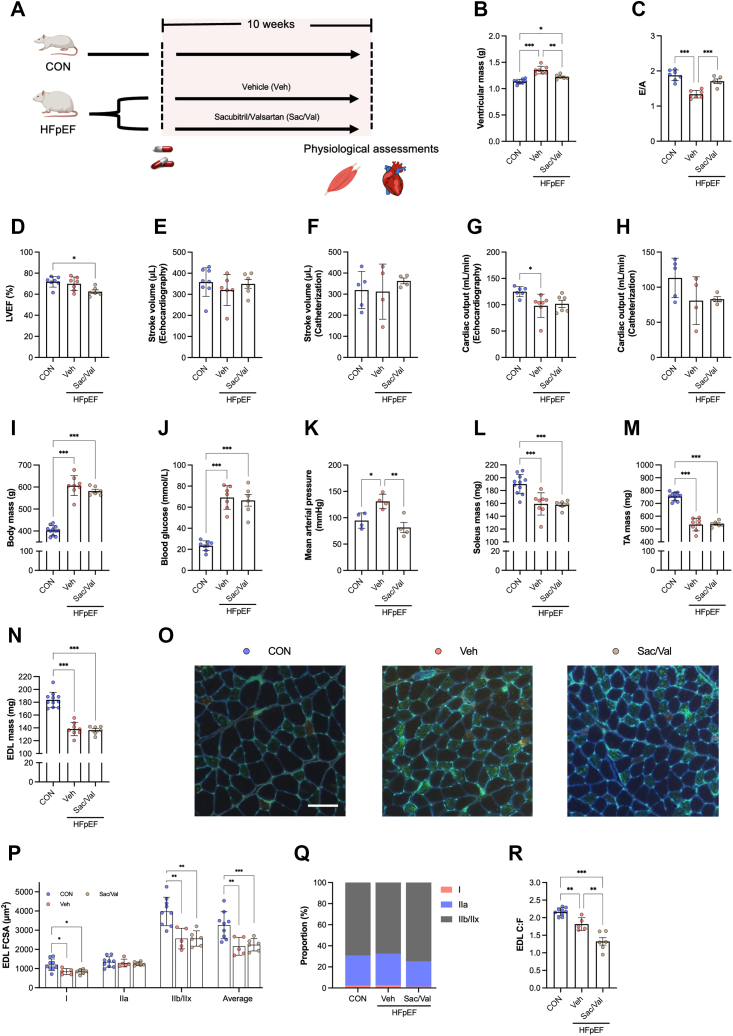
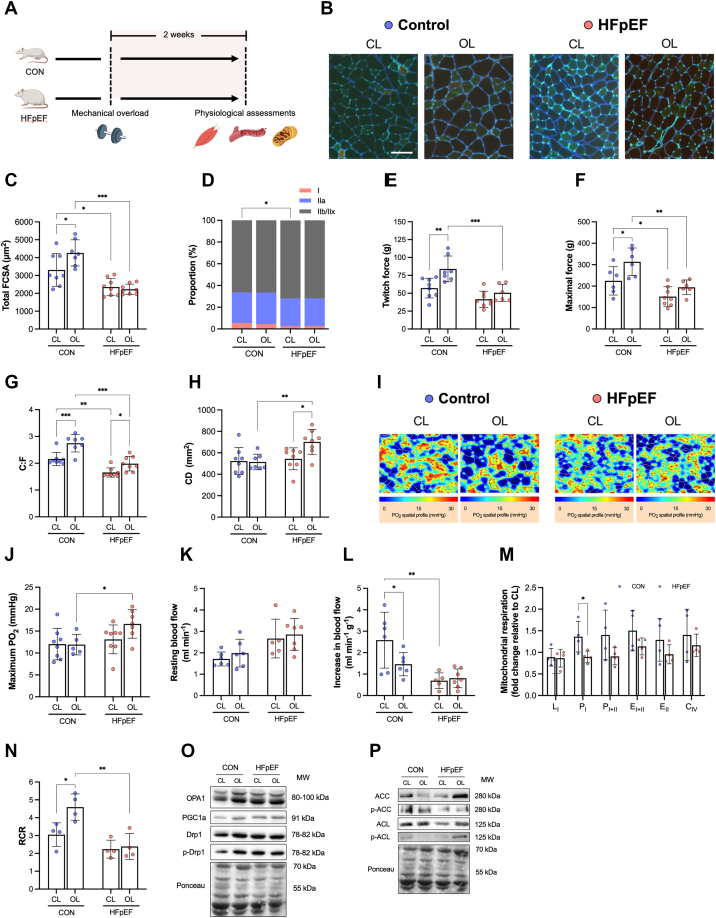
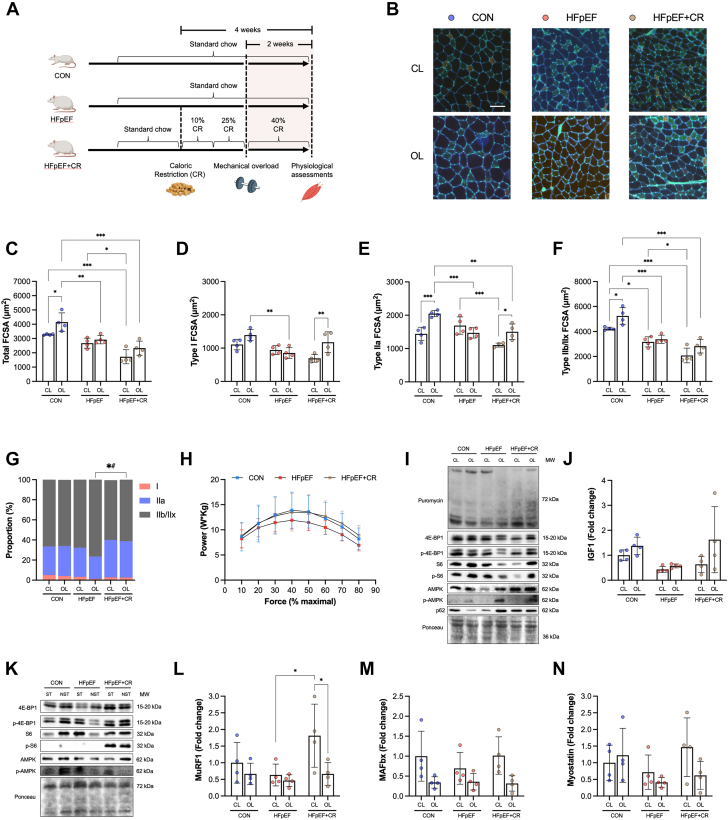
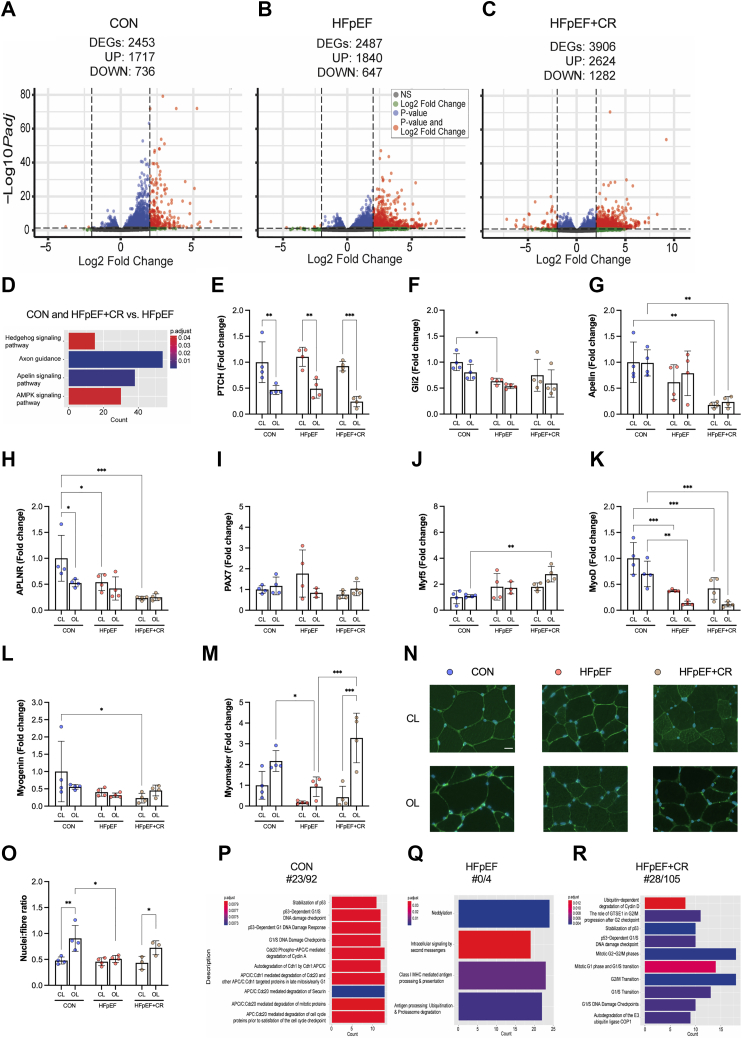
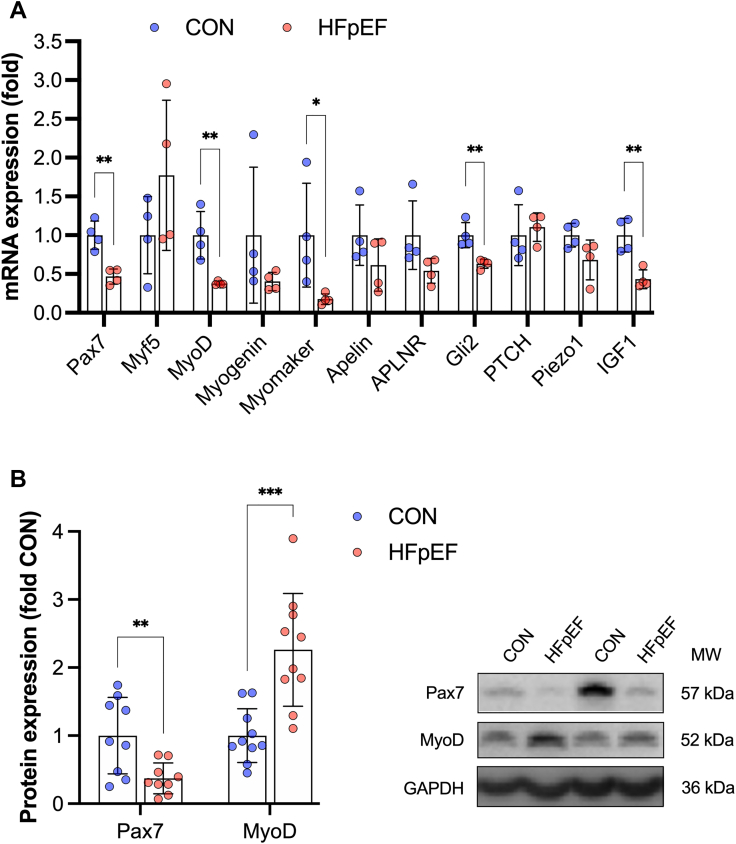
Heart failure with preserved ejection fraction (HFpEF) is a major clinical problem, with limited treatments. HFpEF is characterized by a distinct, but poorly understood, skeletal muscle pathology, which could offer an alternative therapeutic target. In a rat model, we identified impaired myonuclear accretion as a mechanism for low myofiber growth in HFpEF following resistance exercise. Acute caloric restriction rescued skeletal muscle pathology in HFpEF, whereas cardiac therapies had no effect. Mechanisms regulating myonuclear accretion were dysregulated in patients with HFpEF. Overall, these findings may have widespread implications in HFpEF, indicating combined dietary with exercise interventions as a beneficial approach to overcome skeletal muscle pathology.
Keywords: HFpEF; diet; exercise training; mitochondria; skeletal muscle.
© 2024 The Authors.
Conflict of interest statement
Dr Espino-Gonzalez is a recipient of a doctoral fellowship from the Mexican National Council of Science and Technology (CONACYT). Dr Altara’s work was supported by a grant from the K.G. Jebsen Center for Heart Failure Research. Dr Cheng is supported by BHF Mautner Career Development Fellowship. Dr Justo da Silva was supported by the South-Eastern Norway Regional Health Authority (HSØ-RHF, Project No. 25674). Dr Booz has received support from the Pharmacology Clinical Research Core of the University of Mississippi Medical Center School of Medicine. Dr Bowen has received funding from the Medical Research Council (UK) (MR/S025472/1) and Heart Research UK (TRP16/19). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Dunlay S.M., Roger V.L., Redfield M.M. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2017;14:591–602. - PubMed
-
- Gevaert A.B., Kataria R., Zannad F., et al. Heart failure with preserved ejection fraction: recent concepts in diagnosis, mechanisms and management. Heart. 2022;108:1342–1350. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
