

Bilateral erector spinae plane block for postoperative pain relief in lumbar spine surgery: A PRISMA-compliant updated systematic review & meta-analysis
- PMID: 38511162
- PMCID: PMC10950749
- DOI: 10.1016/j.wnsx.2024.100360
Bilateral erector spinae plane block for postoperative pain relief in lumbar spine surgery: A PRISMA-compliant updated systematic review & meta-analysis
Abstract
Study design: Systematic review.
Objective: Erector spinae plane block (ESPB) is growing in popularity over the recent past as an adjuvant modality in multimodal analgesic management following lumbar spine surgery (LSS). The current updated meta-analysis was performed to analyze the efficacy of ESPB for postoperative analgesia in patients undergoing LSS.
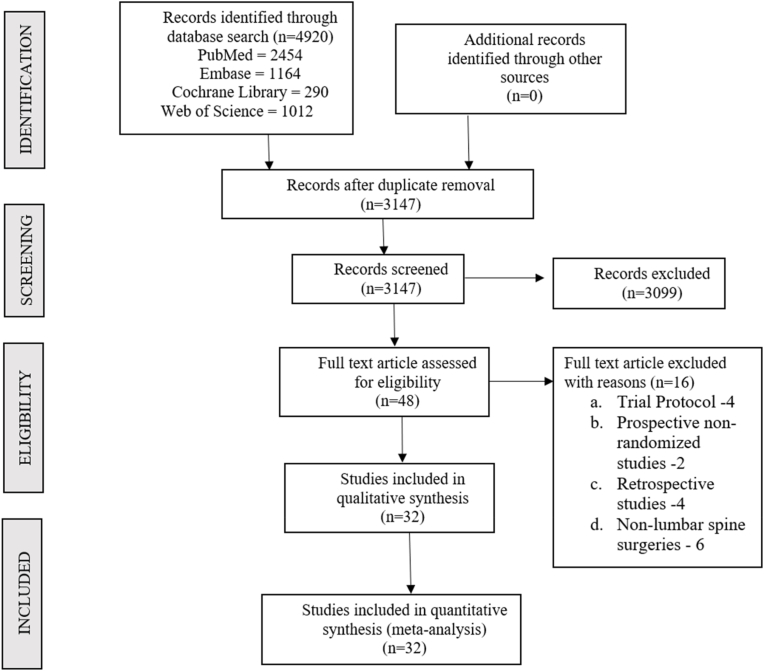
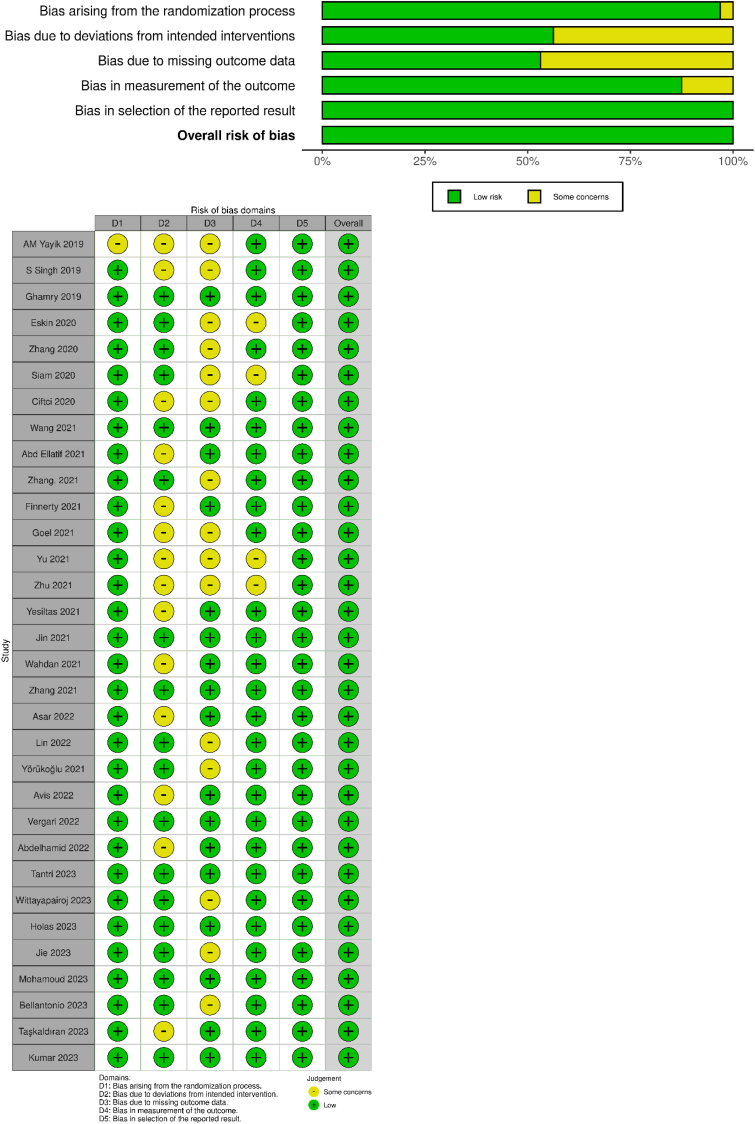
Methods: We conducted independent and duplicate electronic database searches including PubMed, Embase and Cochrane Library till June 2023 for randomized controlled trials (RCTs) analyzing the efficacy of bilateral ESPB for postoperative pain relief in lumbar spine surgeries. Post-operative pain scores, total analgesic consumption, first analgesic requirement time, length of stay and complications were the outcomes evaluated. Statistical analysis was performed using STATA 17 software.
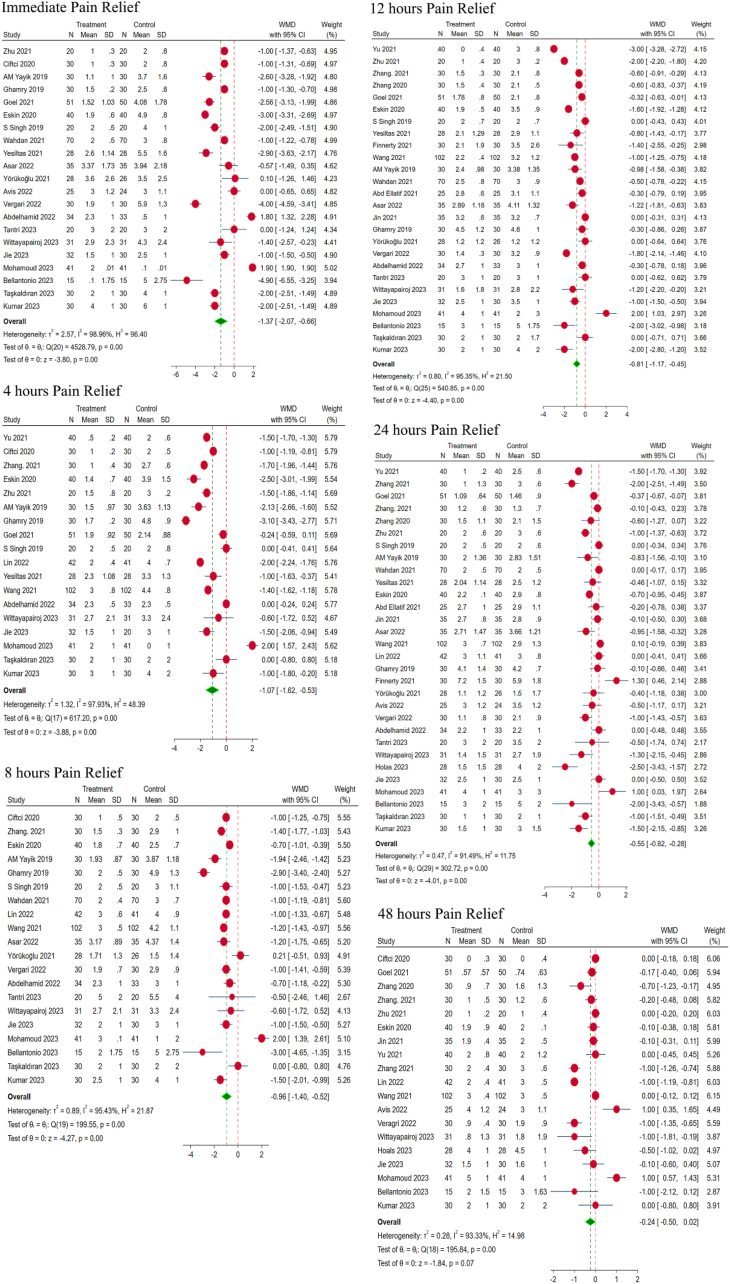
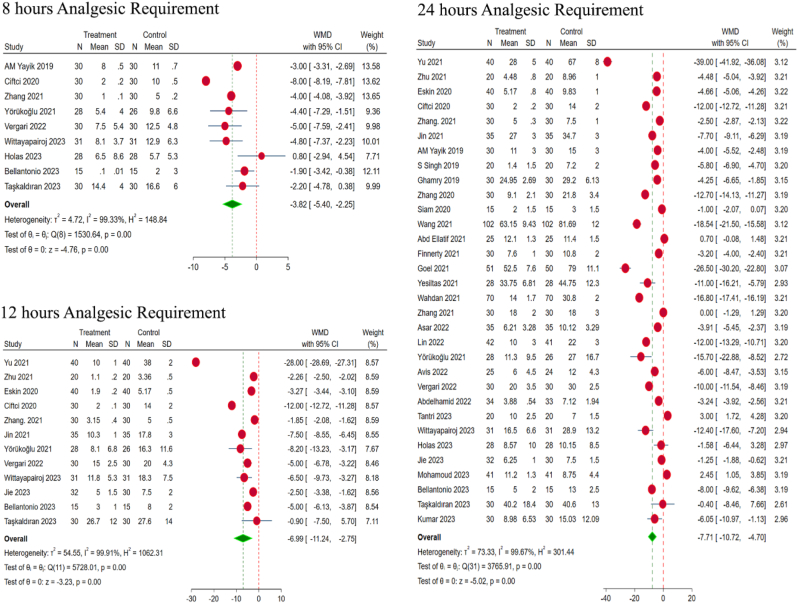
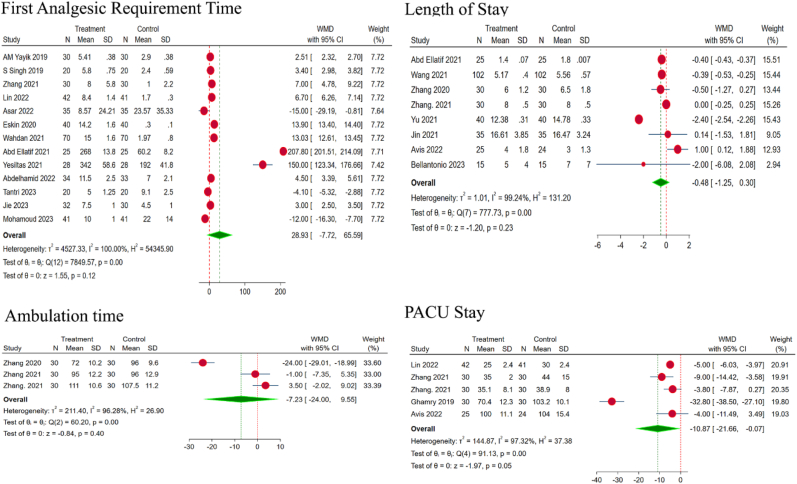
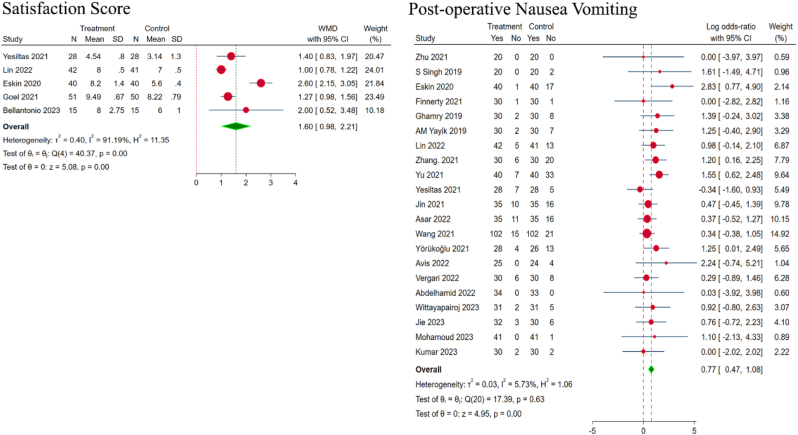
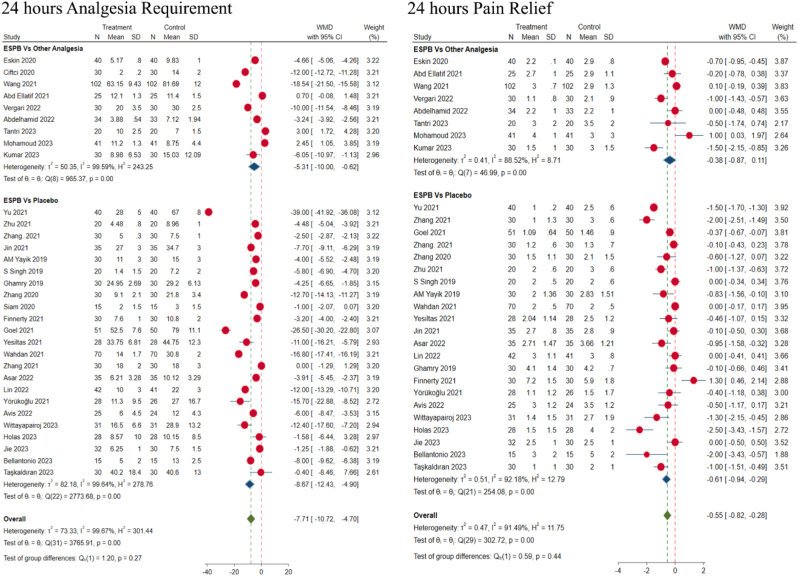
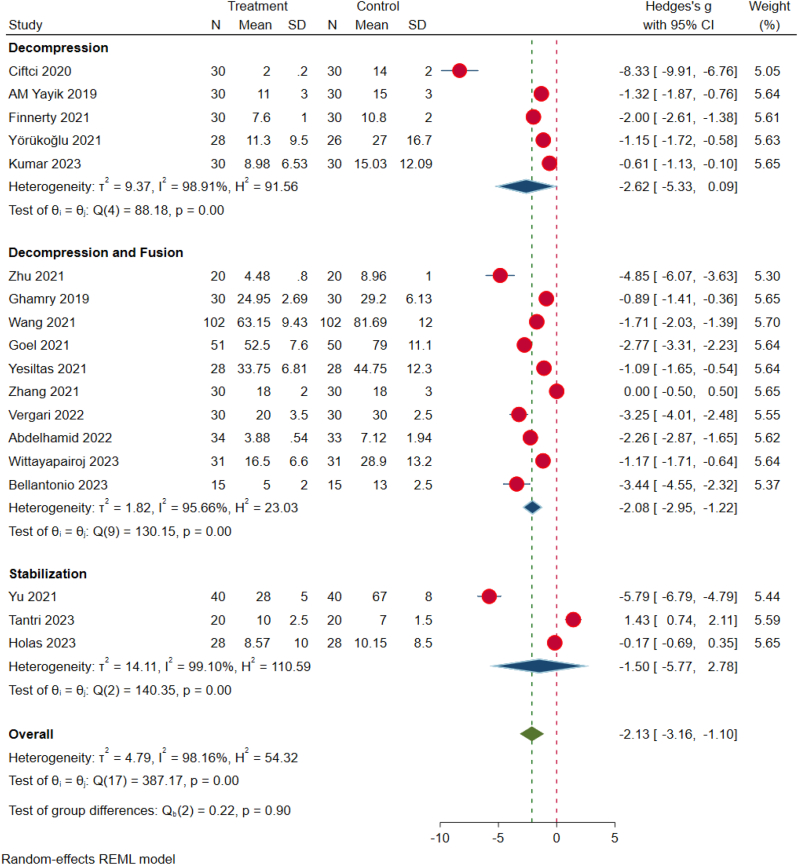
Results: 32 RCTs including 1464 patients (ESPB/Control = 1077/1069) were included in the analysis. There was a significant pain relief in ESPB group, as compared to placebo across all timelines such as during immediate post-operative period (p < 0.001), 4 h (p < 0.001), 8 h (p < 0.001), 12 h (p < 0.001), 24 h (p = 0.001) post-surgery. Similarly, ESPB group showed a significant reduction in analgesic requirement at 8 h (p < 0.001), 12 h (p = 0.001), and 24 h (p < 0.001). However, no difference was noted in the first analgesic requirement time, time to ambulate or total length of stay in the hospital. ESPB demonstrated significantly improved overall satisfaction score for the analgesic management (p < 0.001), reduced intensive care stay (p < 0.05) with significantly reduced post-operative nausea and vomiting (p < 0.001) compared to controls.
Conclusion: ESPB offers prolonged post-operative pain relief compared to controls, thereby reducing the need for opioid consumption and its related complications.
Keywords: Erector spinae plane block; Lumbar spine surgery; Postoperative pain; Regional anaesthesia; Systematic review.
© 2024 The Author(s).
Conflict of interest statement
On behalf of all authors, corresponding author declare no conflict of interest.
Figures
Similar articles
-
Ultrasound-guided erector spinae plane block for postoperative short-term outcomes in lumbar spine surgery: A meta-analysis and systematic review.Medicine (Baltimore). 2023 Feb 17;102(7):e32981. doi: 10.1097/MD.0000000000032981. Medicine (Baltimore). 2023. PMID: 36800574 Free PMC article.
-
Erector spinae plane block for laparoscopic surgeries: a systematic review and meta-analysis.BMC Anesthesiol. 2024 Oct 29;24(1):389. doi: 10.1186/s12871-024-02775-4. BMC Anesthesiol. 2024. PMID: 39472781 Free PMC article.
-
Efficacy and Safety of Erector Spinae Plane Block for Perioperative Pain Management in Lumbar Spinal Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Pain Res. 2023 May 3;16:1453-1475. doi: 10.2147/JPR.S402931. eCollection 2023. J Pain Res. 2023. PMID: 37163199 Free PMC article. Review.
-
Efficacy and Safety of Bilateral Ultrasound-Guided Erector Spinae Plane Block for Postoperative Analgesia in Spine Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.World Neurosurg. 2024 Jan;181:e655-e677. doi: 10.1016/j.wneu.2023.10.111. Epub 2023 Oct 28. World Neurosurg. 2024. PMID: 37898266
-
Postoperative analgesia efficacy of erector spinae plane block in adult abdominal surgery: A systematic review and meta-analysis of randomized trials.Front Med (Lausanne). 2022 Oct 4;9:934866. doi: 10.3389/fmed.2022.934866. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36267624 Free PMC article.
Cited by
-
Impact of Erector Spinae Plane Blocks on Pain Management and Postoperative Outcomes in Patients with Chronic Pain Undergoing Spine Fusion Surgery: A Retrospective Cohort Study.J Pain Res. 2024 Nov 27;17:4023-4031. doi: 10.2147/JPR.S483144. eCollection 2024. J Pain Res. 2024. PMID: 39619213 Free PMC article.
-
Analgesic efficacy and safety of erector spinae plane block versus serratus anterior plane block in breast surgery-a meta-analysis and systematic review of randomized controlled trials.J Anesth Analg Crit Care. 2024 Dec 18;4(1):82. doi: 10.1186/s44158-024-00218-7. J Anesth Analg Crit Care. 2024. PMID: 39695870 Free PMC article. Review.
-
Analgesic effects of erector spinae plane block in patients undergoing nephrectomy: a systematic review and meta-analysis of randomized controlled trials.World J Urol. 2025 May 8;43(1):285. doi: 10.1007/s00345-025-05636-y. World J Urol. 2025. PMID: 40338348
References
-
- Bianconi M., Ferraro L., Ricci R., et al. The pharmacokinetics and efficacy of ropivacaine continuous wound instillation after spine fusion surgery. Anesth Analg. 2004;98:166. - PubMed
-
- Soffin E.M., Beckman J.D., Tseng A., et al. Enhanced recovery after lumbar spine fusion: a randomized controlled trial to assess the quality of patient recovery. Anesthesiology. 2020;133:350–363. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
