

Colchicine's Role in Cardiovascular Disease Management
- PMID: 38511324
- PMCID: PMC11047118
- DOI: 10.1161/ATVBAHA.124.319851
Colchicine's Role in Cardiovascular Disease Management
Erratum in
-
Correction to: Colchicine's Role in Cardiovascular Disease Management.Arterioscler Thromb Vasc Biol. 2024 Jul;44(7):e208. doi: 10.1161/ATV.0000000000000172. Epub 2024 Jun 26. Arterioscler Thromb Vasc Biol. 2024. PMID: 38924445 No abstract available.
Abstract
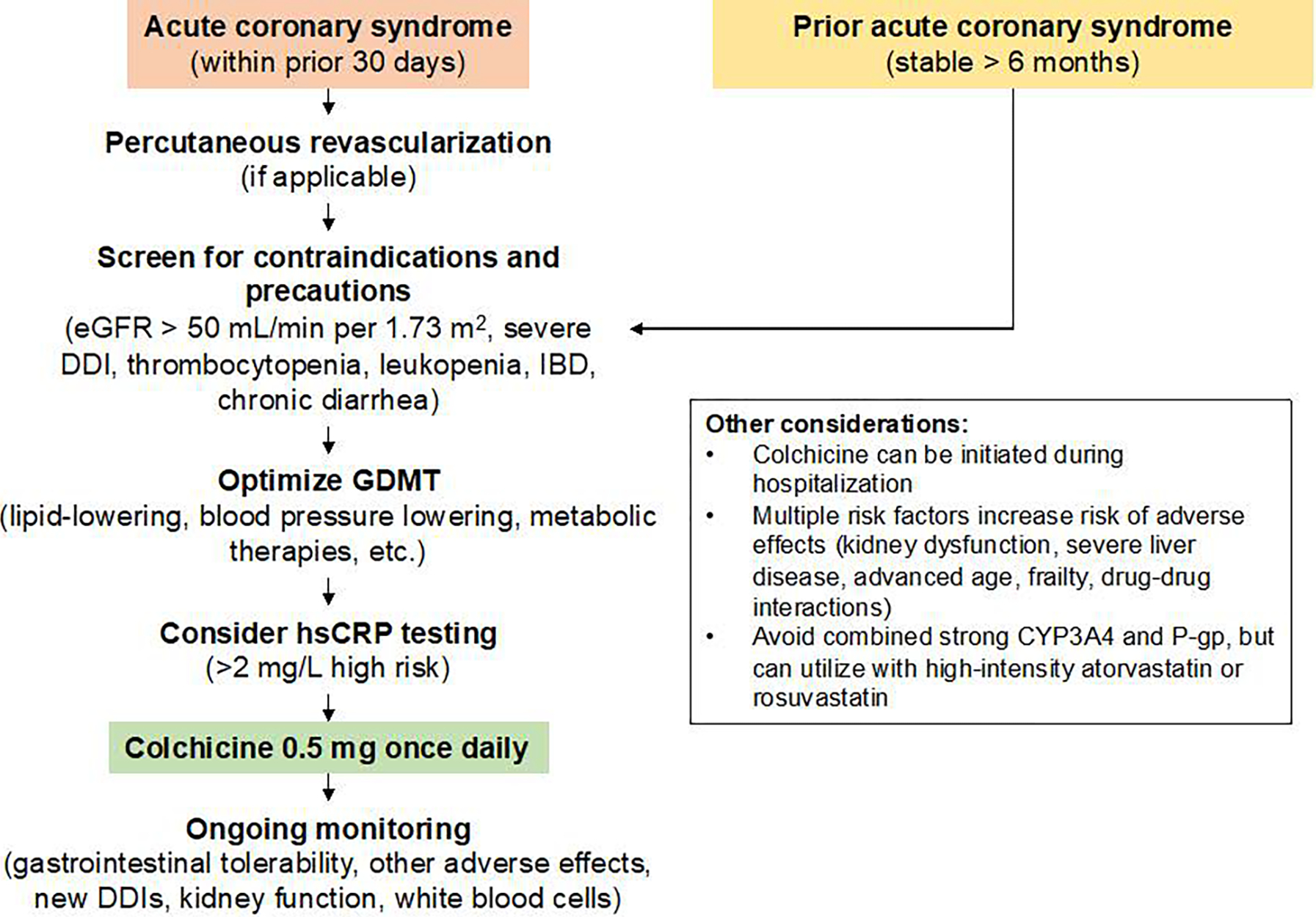
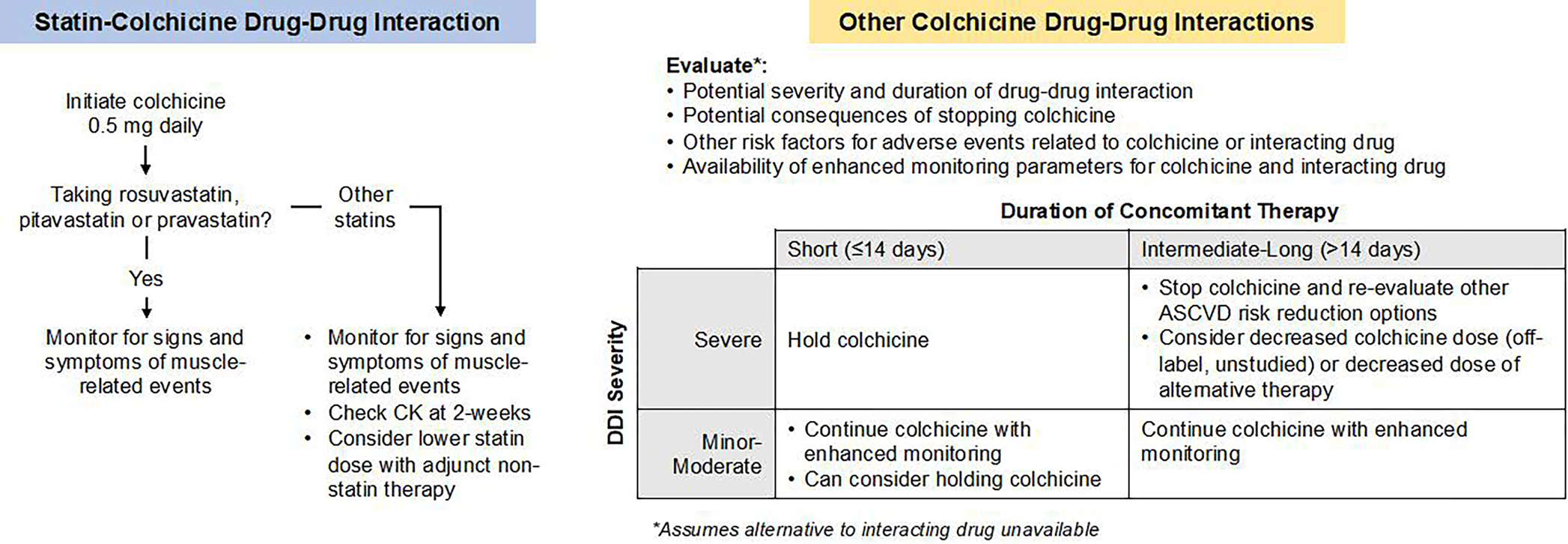
Colchicine-an anti-inflammatory alkaloid-has assumed an important role in the management of cardiovascular inflammation ≈3500 years after its first medicinal use in ancient Egypt. Primarily used in high doses for the treatment of acute gout flares during the 20th century, research in the early 21st century demonstrated that low-dose colchicine effectively treats acute gout attacks, lowers the risk of recurrent pericarditis, and can add to secondary prevention of major adverse cardiovascular events. As the first Food and Drug Administration-approved targeted anti-inflammatory cardiovascular therapy, colchicine currently has a unique role in the management of atherosclerotic cardiovascular disease. The safe use of colchicine requires careful monitoring for drug-drug interactions, changes in kidney and liver function, and counseling regarding gastrointestinal upset. Future research should elucidate the mechanisms of anti-inflammatory effects of colchicine relevant to atherosclerosis, the potential role of colchicine in primary prevention, in other cardiometabolic conditions, colchicine's safety in cardiovascular patients, and opportunities for individualizing colchicine therapy using clinical and molecular diagnostics.
Keywords: cardiovascular system; colchicine; humans; inflammation; kidney; liver.
Conflict of interest statement
Figures




References
-
- Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: Twenty-four-hour outcome of the first multicenter, randomized, double-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum. 2010;62:1060–1068. - PubMed
-
- Dinarello CA, Wolff SM, Goldfinger SE, Dale DC, Alling DW. Colchicine therapy for familial mediterranean fever. A double-blind trial. N Engl J Med. 1974;291:934–937. - PubMed
-
- Chiabrando JG, Bonaventura A, Vecchié A, Wohlford GF, Mauro AG, Jordan JH, Grizzard JD, Montecucco F, Berrocal DH, Brucato A, Imazio M, Abbate A. Management of Acute and Recurrent Pericarditis: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75:76–92. - PubMed
-
- Tardif J-C, Kouz S, Waters DD, Bertrand OF, Diaz R, Maggioni AP, Pinto FJ, Ibrahim R, Gamra H, Kiwan GS, Berry C, López-Sendón J, Ostadal P, Koenig W, Angoulvant D, Grégoire JC, Lavoie M-A, Dubé M-P, Rhainds D, Provencher M, Blondeau L, Orfanos A, L’Allier PL, Guertin M-C, Roubille F. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N Engl J Med. 2019;381:2497–2505. - PubMed
-
- Nidorf SM, Fiolet ATL, Mosterd A, Eikelboom JW, Schut A, Opstal TSJ, The SHK, Xu X-F, Ireland MA, Lenderink T, Latchem D, Hoogslag P, Jerzewski A, Nierop P, Whelan A, Hendriks R, Swart H, Schaap J, Kuijper AFM, van Hessen MWJ, Saklani P, Tan I, Thompson AG, Morton A, Judkins C, Bax WA, Dirksen M, Alings M, Hankey GJ, Budgeon CA, Tijssen JGP, Cornel JH, Thompson PL. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020; - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
