

Invasive Fungal Diseases in Adult Patients in Intensive Care Unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM
- PMID: 38512399
- PMCID: PMC11018656
- DOI: 10.1007/s00134-024-07341-7
Invasive Fungal Diseases in Adult Patients in Intensive Care Unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM
Abstract
Purpose: The aim of this document was to develop standardized research definitions of invasive fungal diseases (IFD) in non-neutropenic, adult patients without classical host factors for IFD, admitted to intensive care units (ICUs).
Methods: After a systematic assessment of the diagnostic performance for IFD in the target population of already existing definitions and laboratory tests, consensus definitions were developed by a panel of experts using the RAND/UCLA appropriateness method.
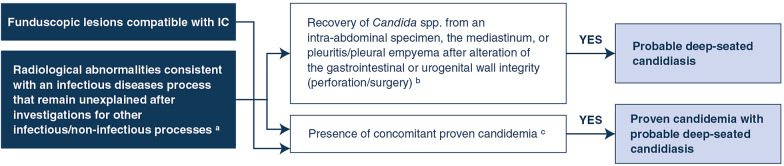
Results: Standardized research definitions were developed for proven invasive candidiasis, probable deep-seated candidiasis, proven invasive aspergillosis, probable invasive pulmonary aspergillosis, and probable tracheobronchial aspergillosis. The limited evidence on the performance of existing definitions and laboratory tests for the diagnosis of IFD other than candidiasis and aspergillosis precluded the development of dedicated definitions, at least pending further data. The standardized definitions provided in the present document are aimed to speed-up the design, and increase the feasibility, of future comparative research studies.
Keywords: Aspergillus; Candida; Consensus; Definitions; Diagnosis; Intensive care unit; Invasive fungal diseases; Research.
© 2024. The Author(s).
Conflict of interest statement
Outside the submitted work, MB reports research grants and/or personal fees for advisor/consultant and/or speaker/chairman from BioMérieux, Cidara, Gilead, Menarini, MSD, Pfizer, and Shionogi. Outside the submitted work, DRG reports investigator-initiated grants from Pfizer Inc, Shionogi, BioMérieux, and Gilead Italia, and personal fees for advisor/speaker from Pfizer Inc., Menarini, and Tillotts Pharma. Outside the submitted work, AAI reports fees for educational lectures from Gilead, Pfizer, and MSD; grants from Instituto de Salud Carlos III and ESCMID; advisor for the Joint Program Initiative on Antimicrobial Resistance and the WHO Technical Expert Group for the Development of the Fungal Priority Pathogens List; travel support from Gilead. Outside the submitted work, EA reports grants from Pfizer and MSD, and honoraria for lectures or presentations from Gilead, Pfizer, Alexion, Mindray, and Sanofi. OAC reports grants or contracts from BMBF, Cidara, EU-DG RTD (101037867), F2G, Gilead, MedPace, MSD, Mundipharma, Octapharma, Pfizer, Scynexis; Consulting fees from Abbvie, AiCuris, Biocon, Cidara, Gilead, IQVIA, Janssen, Matinas, MedPace, Menarini, Moderna, Molecular Partners, MSG-ERC, Noxxon, Octapharma, Pfizer, PSI, Scynexis, Seres; honoraria for lectures from Abbot, Abbvie, Al-Jazeera Pharmaceuticals/Hikma Gilead, Grupo Biotascana/United Medical/Knight ISHAM Working group, MedScape, MedUpdate, Merck/MSD, Noscendo, Pfizer,Shionogi, StreamedUp; payment for expert testimony from Cidara; Participation on a Data Safety Monitoring Board or Advisory Board from Boston Strategic Partners, Cidara, IQVIA, Janssen, MedPace, Pulmocide, Shionogi, PSI, The Prime Meridian Group; a pending patent currently reviewed at the German Patent and Trade Mark Office; stoke or stoke options from CoRe Consulting and EasyRadiology; other interests from Wiley, outside the submitted work. Outside the submitted work, FGDR reports consulting fess/honoraria for lectures from MSD, Pfizer, and Gilead Sciences, and travel fees from Pfizer and MSD. JDW reports grants for advisor/consultant or speaker/chairman from for MSD, Pfizer, and ThermoFisher (fees and honoraria paid to institution). GD reports honoraria for lectures/presentations from Gilead, Pfizer, and InfectoPharm. JGM reports personal fees for advisor/consultant and/or speaker/chairman from Gilead and Pfizer. MH received research funding from Gilead Sciences, Astellas, Mundipharma, Euroimmune, MSD, Pulmocide, IMMY, Scynexis, F2G and Pfizer, outside the submitted work. Outside the submitted work, SSK reports fees for lectures/advisory board from Basilea, MSD, Pfizer, and Hikma. PK reports grants or contracts from German Federal Ministry of Research and Education (BMBF) B-FAST (Bundesweites Forschungsnetz Angewandte Surveillance und Testung) and NAPKON (Nationales Pandemie Kohorten Netz, German National Pandemic Cohort Network) of the Network University Medicine (NUM) and the State of North Rhine-Westphalia; consulting fees Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited, Noxxon N.V. and Pfizer Pharma; honoraria for lectures from Akademie für Infektionsmedizin e.V., Ambu GmbH, Astellas Pharma, BioRad Laboratories Inc., Datamed GmbH, European Confederation of Medical Mycology, Gilead Sciences, GPR Academy Ruesselsheim, HELIOS Kliniken GmbH, Lahn-Dill-Kliniken GmbH, medupdate GmbH, MedMedia GmbH, MSD Sharp & Dohme GmbH, Pfizer Pharma GmbH, Scilink Comunicación Científica SC and University Hospital and LMU Munich; participation on an Advisory Board from Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited and Pfizer Pharma; a pending patent currently reviewed at the German Patent and Trade Mark Office (DE 10 2021 113 007.7); other non-financial interests from Elsevier, Wiley and Taylor & Francis online outside the submitted work. Outside the submitted work, FL reports grants from Pfizer, Gilead, MSD, Novartis, Swiss National Science Foundation, Santos-Suarez Foundation; and honoraria for lectures/presentation from Gilead, Pfizer, MSD, Mundipharma. Outside the submitted work, CLF reports research grants and/or personal fees for advisor/consultant, travel and/or speaker/chairman from Gilead, MSD, Pfizer, BioMérieux, F2G, IMMY, Shionogi, Astellas Pharma. Outside the submitted work, JM reports research grants and/or personal fees for advisor/consultant, and/or speaker/chairman from Gilead Sciences, F2G, Shionogi, Mundipharma, Mundipharma, Takeda, and Basilea. Outside the submitted work, IML reports grants from Grifols; consulting fees from MSD, Gilead, Mundipharma, fees for lectures/advisory board from Gilead, MSD, and Mundipharma; travel support from the European Respiratory Society (Chair Critical Care Group). Outside the submitted work, PM reports fees for lectures/advisory board from Gilead, MSD, Mundipharma, Pfizer. Outside of the submitted work, GP reports fees for lectures/advisory board from AstraZeneca, Gilead, Glaxo, Menarini, MSD, Pfizer and SOBI; grants from Adagio Therapeutics, AstraZeneca, Bausch, Fabentech, Pfizer, PharmaMar, Roche, Xenothera. Outside the submitted work, JR reports consulting fees from Pfizer; honoraria for lectures/presentations from Pfizer, MSD, and Roche; travel support from Roche. Outside the submitted work, J-FT reports grants from Pfizer and MSD; consulting fees from Gilead; honoraria for lectures/presentations from Mundipharma, Gilead, and Pfizer; Advisor fees from MSD, Pfizer, BD, Aspen, Roche diagnostic, and BioMérieux. Outside the submitted work, AT reports consultant/speaker fees from Pfizer, Poliphor, MSD, Jansen, and OM Pharma. Outside the submitted work, JAV reports consulting fees from F2G and Cidara; honoraria for lectures/presentations from Melinta. Outside the submitted work, JW reports investigator-initiated research grants, speaker honoraria and travel grants from Pfizer and Gilead. Outside the submitted work, AC reports fees for lectures/advisory board from Gilead, MSD, Mundipharma, Pfizer. Outside the submitted work, IK reports grants and honoraria for lectures/presentations from Pfizer and BioMérieux. Outside the submitted work, TM reports consultancy fees from Gilead Sciences, Pfizer and AstraZeneca, unrestricted research grants from Gilead Sciences, and travel support from AstraZeneca. Outside the submitted work, KM reports travel support from Gilead. Outside the submitted work, MP reports honoraria for lectures/presentations from Dia Sorin, MDS, Menarini, Pfizer, and ThermoFisher. Outside the submitted work, LS reports travel support from ESCMID. TC has participated in advisory/safety monitoring boards or consulted for Cidara, Novartis, MSD Merck Sharp & Dohme AG, Shionogi and Gilead and received grant from European Community (Horizon 2020, HDM-FUN Grant; host-directed medicine in invasive fungal infections, co-applicant) for projects unrelated to the submitted work; all contracts were made with and fees paid to his institution (CHUV).
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
