

Plasma Proteome-Based Test for First-Line Treatment Selection in Metastatic Non-Small Cell Lung Cancer
- PMID: 38513170
- PMCID: PMC10965206
- DOI: 10.1200/PO.23.00555
Plasma Proteome-Based Test for First-Line Treatment Selection in Metastatic Non-Small Cell Lung Cancer
Abstract
Purpose: Current guidelines for the management of metastatic non-small cell lung cancer (NSCLC) without driver mutations recommend checkpoint immunotherapy with PD-1/PD-L1 inhibitors, either alone or in combination with chemotherapy. This approach fails to account for individual patient variability and host immune factors and often results in less-than-ideal outcomes. To address the limitations of the current guidelines, we developed and subsequently blindly validated a machine learning algorithm using pretreatment plasma proteomic profiles for personalized treatment decisions.
Patients and methods: We conducted a multicenter observational trial (ClinicalTrials.gov identifier: NCT04056247) of patients undergoing PD-1/PD-L1 inhibitor-based therapy (n = 540) and an additional patient cohort receiving chemotherapy (n = 85) who consented to pretreatment plasma and clinical data collection. Plasma proteome profiling was performed using SomaScan Assay v4.1.
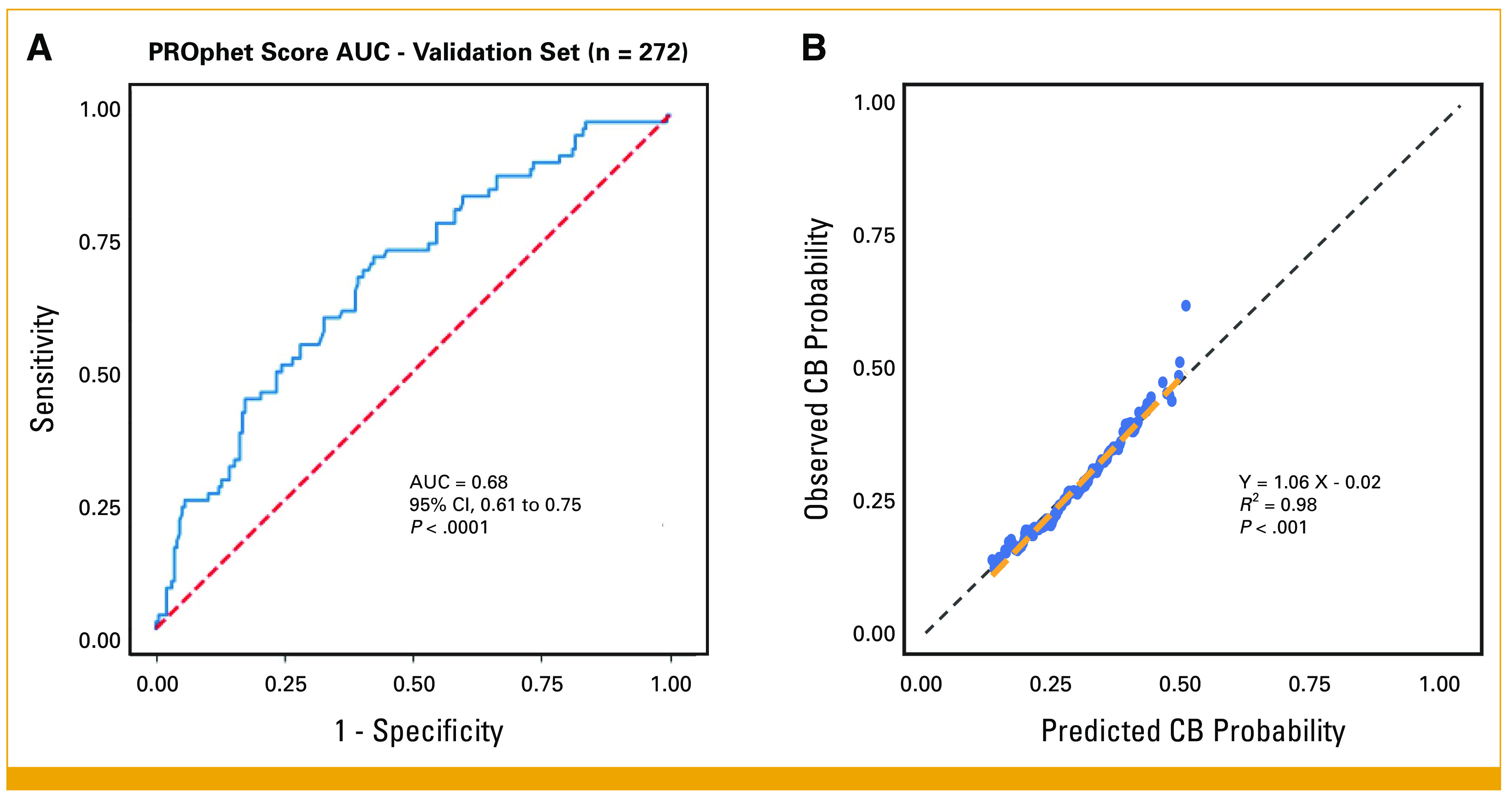
Results: Our test demonstrates a strong association between model output and clinical benefit (CB) from PD-1/PD-L1 inhibitor-based treatments, evidenced by high concordance between predicted and observed CB (R2 = 0.98, P < .001). The test categorizes patients as either PROphet-positive or PROphet-negative and further stratifies patient outcomes beyond PD-L1 expression levels. The test successfully differentiates between PROphet-negative patients exhibiting high tumor PD-L1 levels (≥50%) who have enhanced overall survival when treated with a combination of immunotherapy and chemotherapy compared with immunotherapy alone (hazard ratio [HR], 0.23 [95% CI, 0.1 to 0.51], P = .0003). By contrast, PROphet-positive patients show comparable outcomes when treated with immunotherapy alone or in combination with chemotherapy (HR, 0.78 [95% CI, 0.42 to 1.44], P = .424).
Conclusion: Plasma proteome-based testing of individual patients, in combination with standard PD-L1 testing, distinguishes patient subsets with distinct differences in outcomes from PD-1/PD-L1 inhibitor-based therapies. These data suggest that this approach can improve the precision of first-line treatment for metastatic NSCLC.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures



References
-
- Gaissmaier L, Christopoulos P: Immune modulation in lung cancer: Current concepts and future strategies. Respiration 99:903-929, 2020 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
