

Community based complex interventions to sustain independence in older people: systematic review and network meta-analysis
- PMID: 38514079
- PMCID: PMC10955723
- DOI: 10.1136/bmj-2023-077764
Community based complex interventions to sustain independence in older people: systematic review and network meta-analysis
Abstract
Objective: To synthesise evidence of the effectiveness of community based complex interventions, grouped according to their intervention components, to sustain independence for older people.
Design: Systematic review and network meta-analysis.
Data sources: Medline, Embase, CINAHL, PsycINFO, CENTRAL, clinicaltrials.gov, and International Clinical Trials Registry Platform from inception to 9 August 2021 and reference lists of included studies.
Eligibility criteria: Randomised controlled trials or cluster randomised controlled trials with ≥24 weeks' follow-up studying community based complex interventions for sustaining independence in older people (mean age ≥65 years) living at home, with usual care, placebo, or another complex intervention as comparators.
Main outcomes: Living at home, activities of daily living (personal/instrumental), care home placement, and service/economic outcomes at 12 months.
Data synthesis: Interventions were grouped according to a specifically developed typology. Random effects network meta-analysis estimated comparative effects; Cochrane's revised tool (RoB 2) structured risk of bias assessment. Grading of recommendations assessment, development and evaluation (GRADE) network meta-analysis structured certainty assessment.
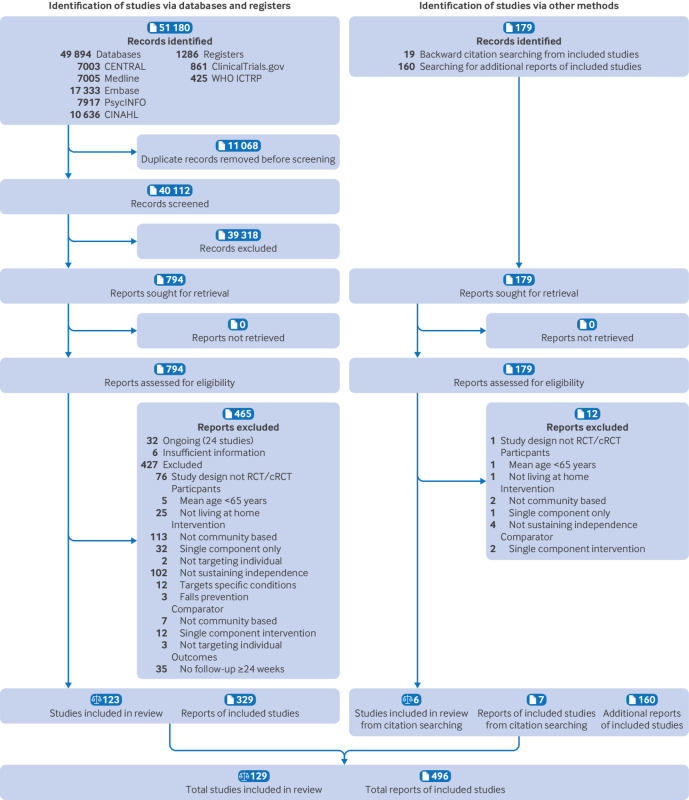
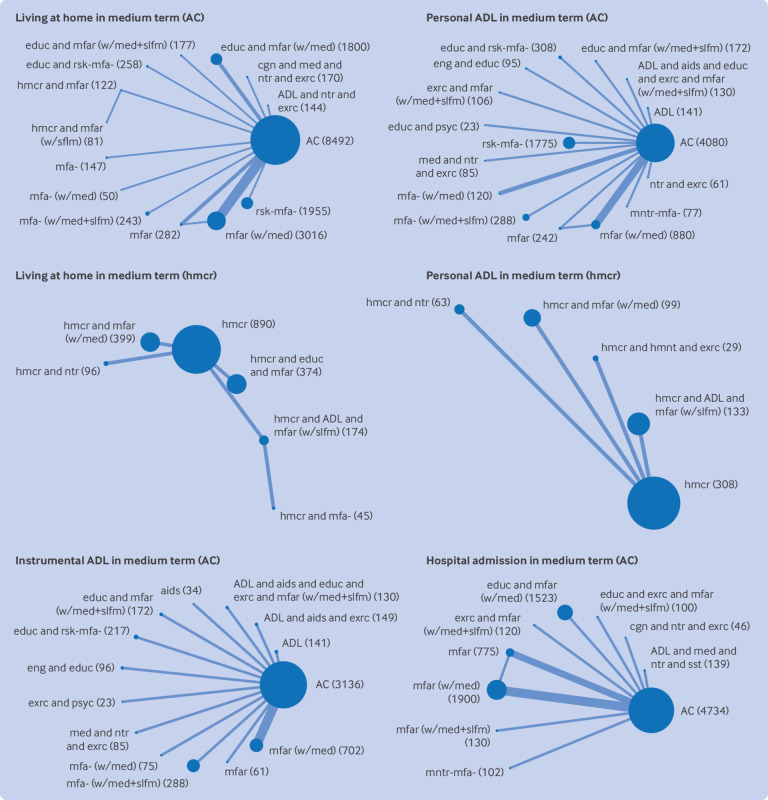
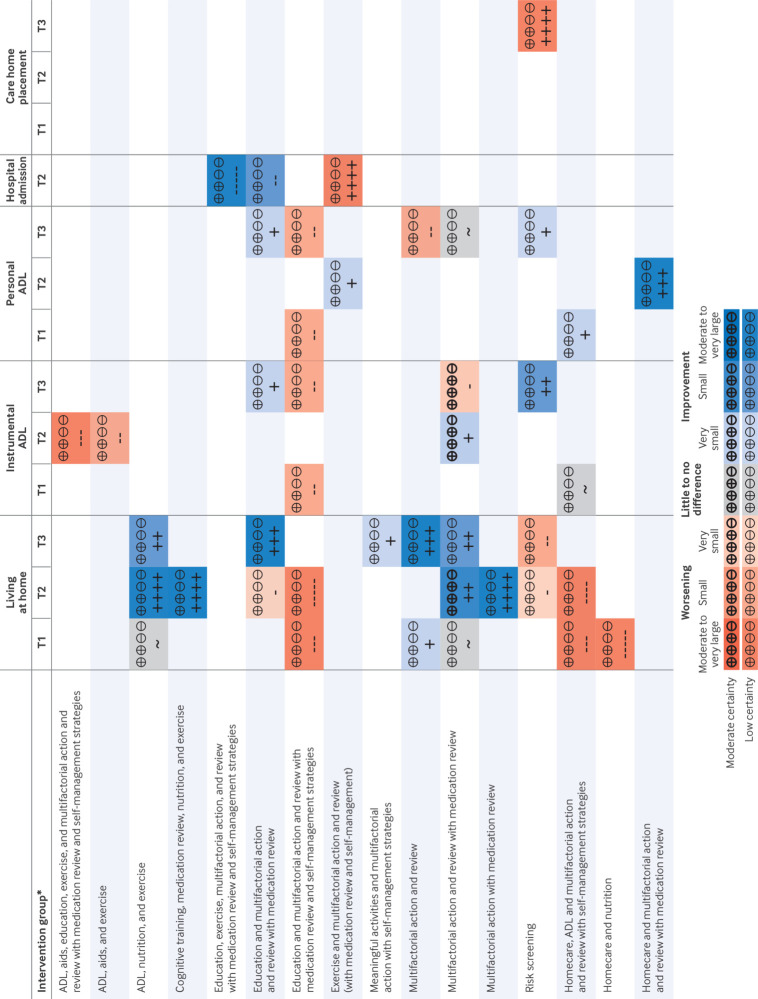
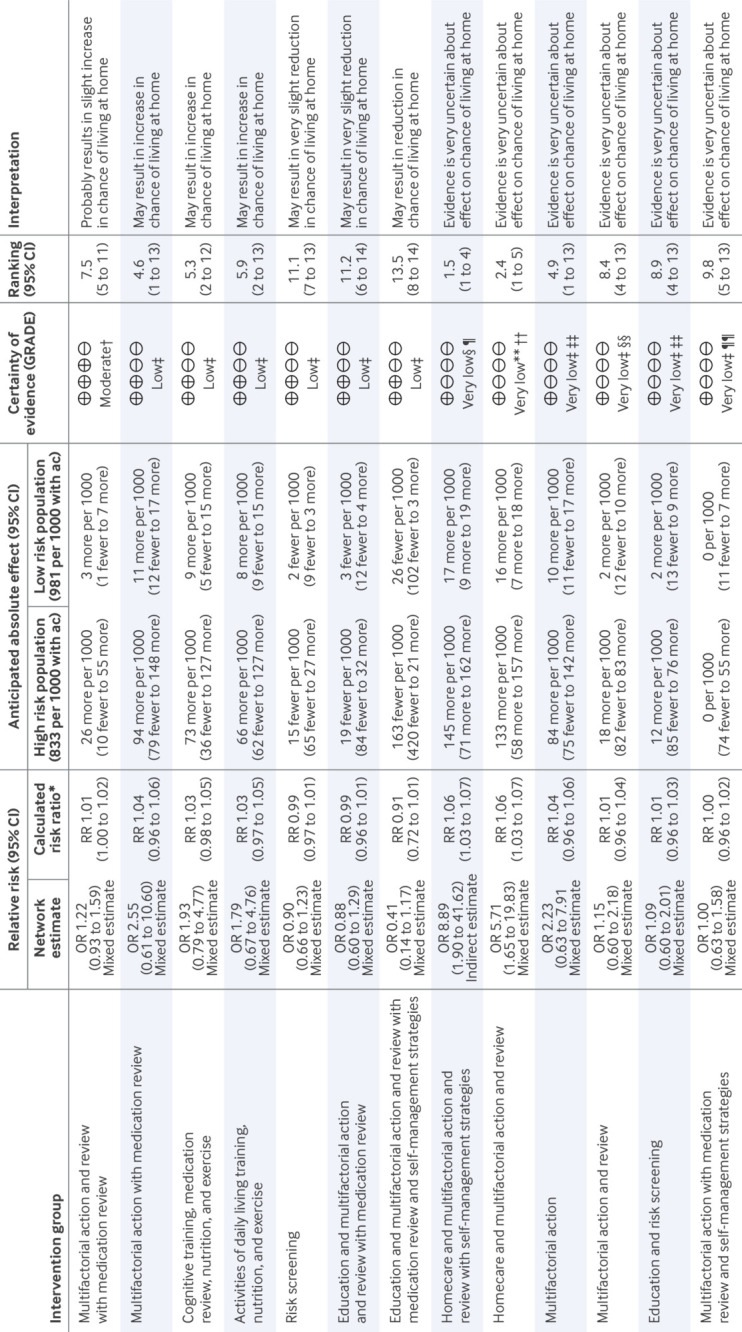
Results: The review included 129 studies (74 946 participants). Nineteen intervention components, including "multifactorial action from individualised care planning" (a process of multidomain assessment and management leading to tailored actions), were identified in 63 combinations. For living at home, compared with no intervention/placebo, evidence favoured multifactorial action from individualised care planning including medication review and regular follow-ups (routine review) (odds ratio 1.22, 95% confidence interval 0.93 to 1.59; moderate certainty); multifactorial action from individualised care planning including medication review without regular follow-ups (2.55, 0.61 to 10.60; low certainty); combined cognitive training, medication review, nutritional support, and exercise (1.93, 0.79 to 4.77; low certainty); and combined activities of daily living training, nutritional support, and exercise (1.79, 0.67 to 4.76; low certainty). Risk screening or the addition of education and self-management strategies to multifactorial action from individualised care planning and routine review with medication review may reduce odds of living at home. For instrumental activities of daily living, evidence favoured multifactorial action from individualised care planning and routine review with medication review (standardised mean difference 0.11, 95% confidence interval 0.00 to 0.21; moderate certainty). Two interventions may reduce instrumental activities of daily living: combined activities of daily living training, aids, and exercise; and combined activities of daily living training, aids, education, exercise, and multifactorial action from individualised care planning and routine review with medication review and self-management strategies. For personal activities of daily living, evidence favoured combined exercise, multifactorial action from individualised care planning, and routine review with medication review and self-management strategies (0.16, -0.51 to 0.82; low certainty). For homecare recipients, evidence favoured addition of multifactorial action from individualised care planning and routine review with medication review (0.60, 0.32 to 0.88; low certainty). High risk of bias and imprecise estimates meant that most evidence was low or very low certainty. Few studies contributed to each comparison, impeding evaluation of inconsistency and frailty.
Conclusions: The intervention most likely to sustain independence is individualised care planning including medicines optimisation and regular follow-up reviews resulting in multifactorial action. Homecare recipients may particularly benefit from this intervention. Unexpectedly, some combinations may reduce independence. Further research is needed to investigate which combinations of interventions work best for different participants and contexts.
Registration: PROSPERO CRD42019162195.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: AC, TC, JE, AF, JGl, MJ, NL, and RRi had financial support from the NIHR Health Technology Assessment Programme for the submitted work; MB had financial support from the PhD Graduate Teaching Fund at the University of Liverpool for the submitted work; DA declares payment made to her employer, University of Leeds Library, from the Academic Unit for Ageing and Stroke Research, Bradford Institute for Health Research, for services that included contributions to the submitted work; TC, AC, and AF received research funding from NIHR Programme Grants for Applied Research; AC and AF also received research funding from NIHR HSDR Programme; AC also received research funding from Health Data Research UK, NIHR ARC Yorkshire and Humber, NIHR Leeds BRC, and Dunhill Medical Trust; AF also declares NIHR Senior Investigator award, National Institute for Health (USA) payment for panel membership in 2021 and 2022, and University of Leeds Governor representative on the Governors Board of Bradford Teaching Hospitals NHS Foundation Trust; MB and MP received NIHR pre-doctoral fellowship funding; RB is supported by matched funding awarded to the NIHR Applied Research Collaboration (West Midlands) and is a member of the data monitoring committee for the Predict and Prevent AECOPD Trial and College of Experts, Versus Arthritis; AC is a member of NIHR HTA Commissioned Research Funding Committee and Dunhill Medical Trust Research Grants Committee; RRi received personal payments for training courses provided in-house to universities (Leeds, Aberdeen, Exeter, LSHTM) and other organisations (Roche), has received personal payments from the BMJ and BMJ Medicine as their statistical editor, is a co-convenor of the Cochrane Prognosis Methods Group and on the Editorial Board of Diagnostic and Prognostic Research, and Research Synthesis Methods, but receives no income for these roles, receives personal payment for being the external examiner of the MSc Medical Statistics, London School of Hygiene and Tropical Medicine, was previously an external examiner for the MSc Medical Statistics at University of Leicester, has written two textbooks for which he receives royalties from sales (Prognosis Research in Healthcare, and Individual Participant Data Meta-analysis), is a lead editor on an upcoming book (Cochrane Handbook for Prognosis Reviews, Wiley, 2025), for which he will receive royalties from sales, has received consulting fees for a training course on IPD meta-analysis from Roche in 2018, the NIHR HTA grant paid for travel to Leeds for one meeting, and is a member of the NIHR Doctoral Research Fellowships grant panel, and a member of the MRC Better Methods Better Research grant panel—for the latter, he receives an attendance fee; MH declares NIHR Academic Clinical Fellowship; OT declares NIHR Academic Clinical Lectureship and Dunhill Medical Trust Doctoral Research Fellowship RTF107/0117; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Maintaining independence in older adults.BMJ. 2024 Mar 21;384:q592. doi: 10.1136/bmj.q592. BMJ. 2024. PMID: 38514071 No abstract available.
-
Patient centred outcomes should be focus of interventions to sustain independence in older people.BMJ. 2024 Apr 24;385:q931. doi: 10.1136/bmj.q931. BMJ. 2024. PMID: 38658034 No abstract available.
References
-
- United Nations Department of Economic and Social Affairs. Population Division. World Population Prospects 2022: Summary of Results. 2022. https://www.un.org/development/desa/pd/sites/www.un.org.development.desa....
-
- World Health Organization. Decade of Healthy Ageing: 2020-2030. https://www.who.int/ageing/decade-of-healthy-ageing.
-
- World Health Organization. Global Health Estimates: Life expectancy and leading causes of death and disability. 2023. https://www.who.int/data/gho/data/themes/mortality-and-global-health-est....
-
- Whitty CJM. Chief medical officer’s annual report 2023: Health in an ageing society. 2023. https://www.gov.uk/government/publications/chief-medical-officers-annual....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources