

Clinicoradiological and neuropathological evaluation of primary progressive aphasia
- PMID: 38514176
- PMCID: PMC11330364
- DOI: 10.1136/jnnp-2023-332862
Clinicoradiological and neuropathological evaluation of primary progressive aphasia
Abstract
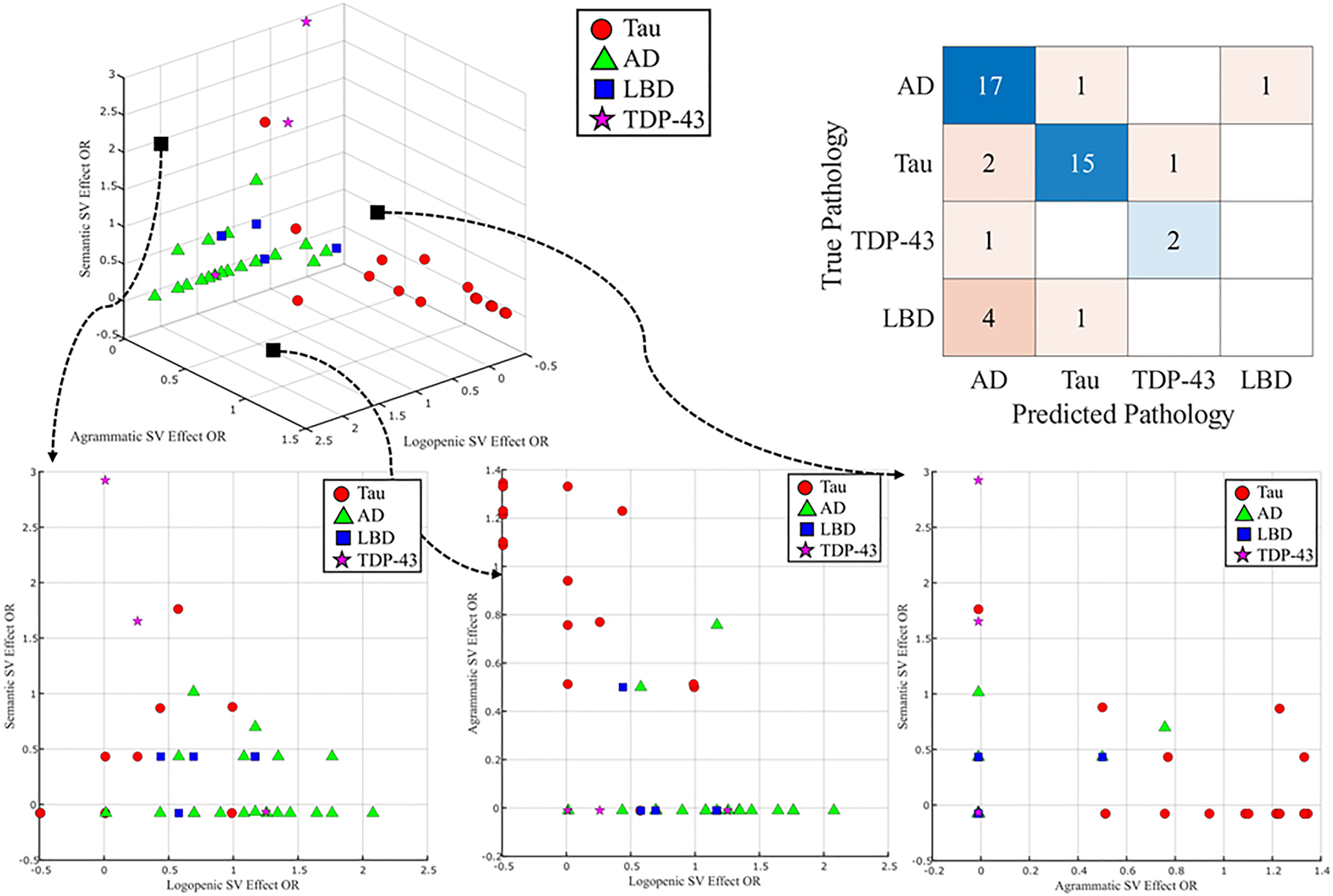
Background: Primary progressive aphasia (PPA) defines a group of neurodegenerative disorders characterised by language decline. Three PPA variants correlate with distinct underlying pathologies: semantic variant PPA (svPPA) with transactive response DNA-binding protein of 43 kD (TDP-43) proteinopathy, agrammatic variant PPA (agPPA) with tau deposition and logopenic variant PPA (lvPPA) with Alzheimer's disease (AD). Our objectives were to differentiate PPA variants using clinical and neuroimaging features, assess progression and evaluate structural MRI and a novel 18-F fluorodeoxyglucose positron emission tomography (FDG-PET) image decomposition machine learning algorithm for neuropathology prediction.
Methods: We analysed 82 autopsied patients diagnosed with PPA from 1998 to 2022. Clinical histories, language characteristics, neuropsychological results and brain imaging were reviewed. A machine learning framework using a k-nearest neighbours classifier assessed FDG-PET scans from 45 patients compared with a large reference database.
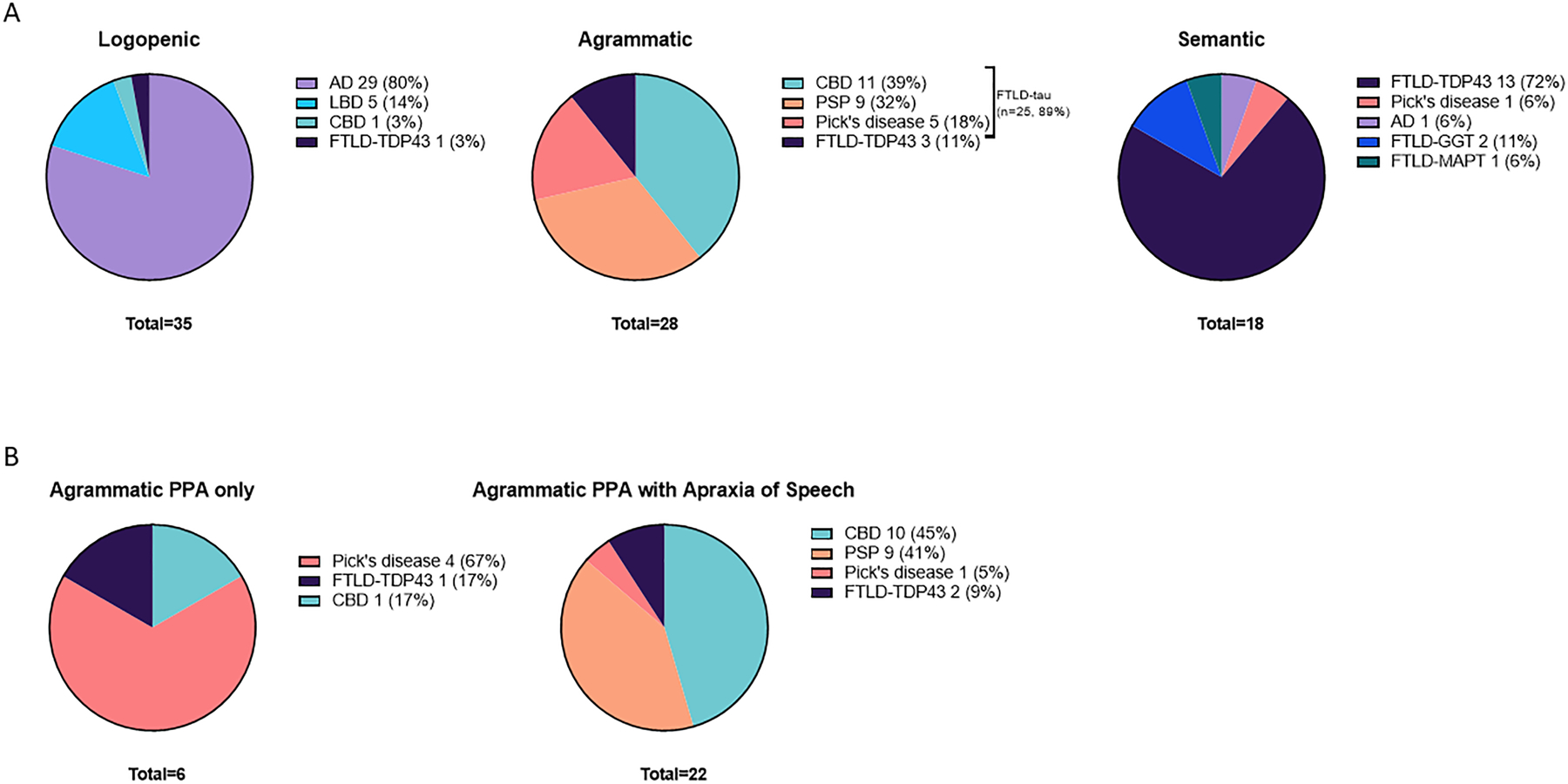
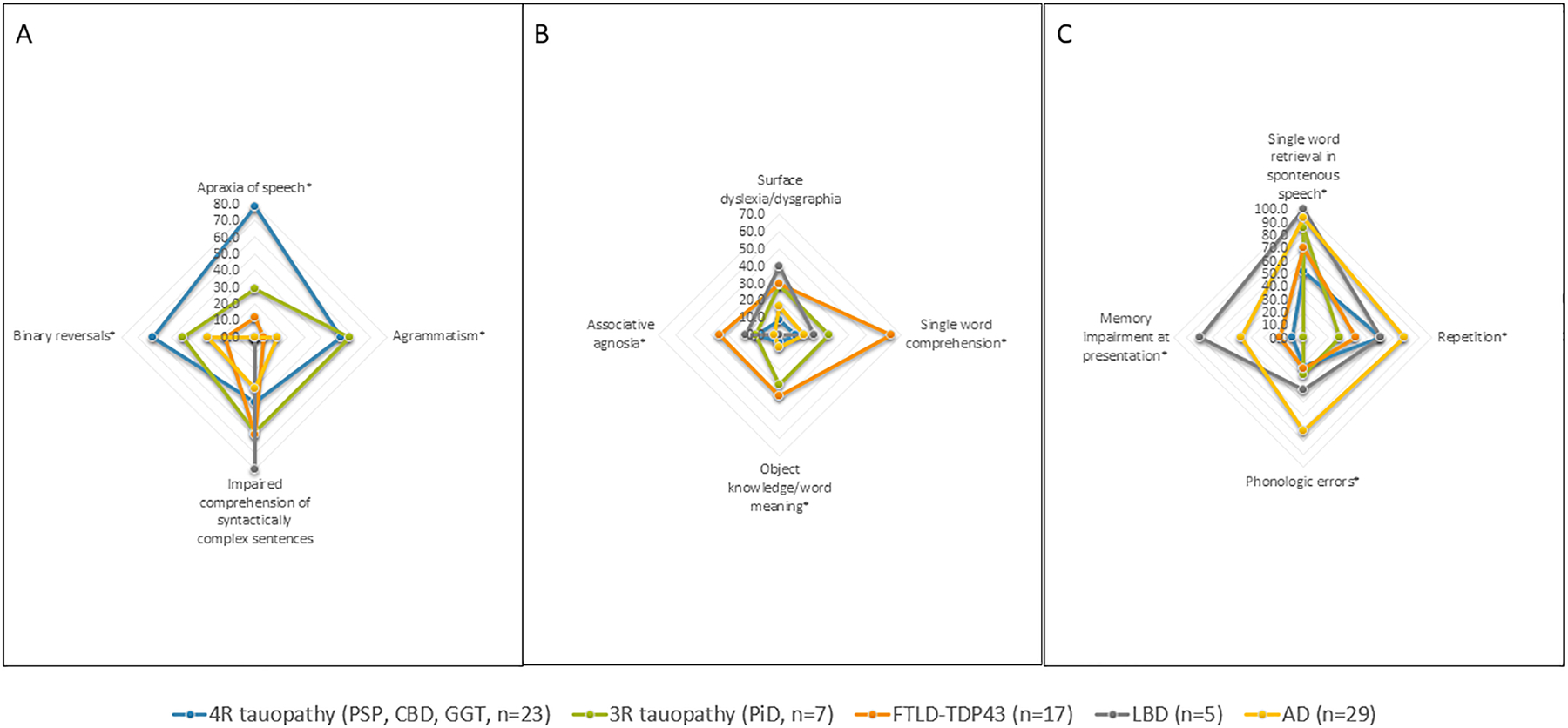
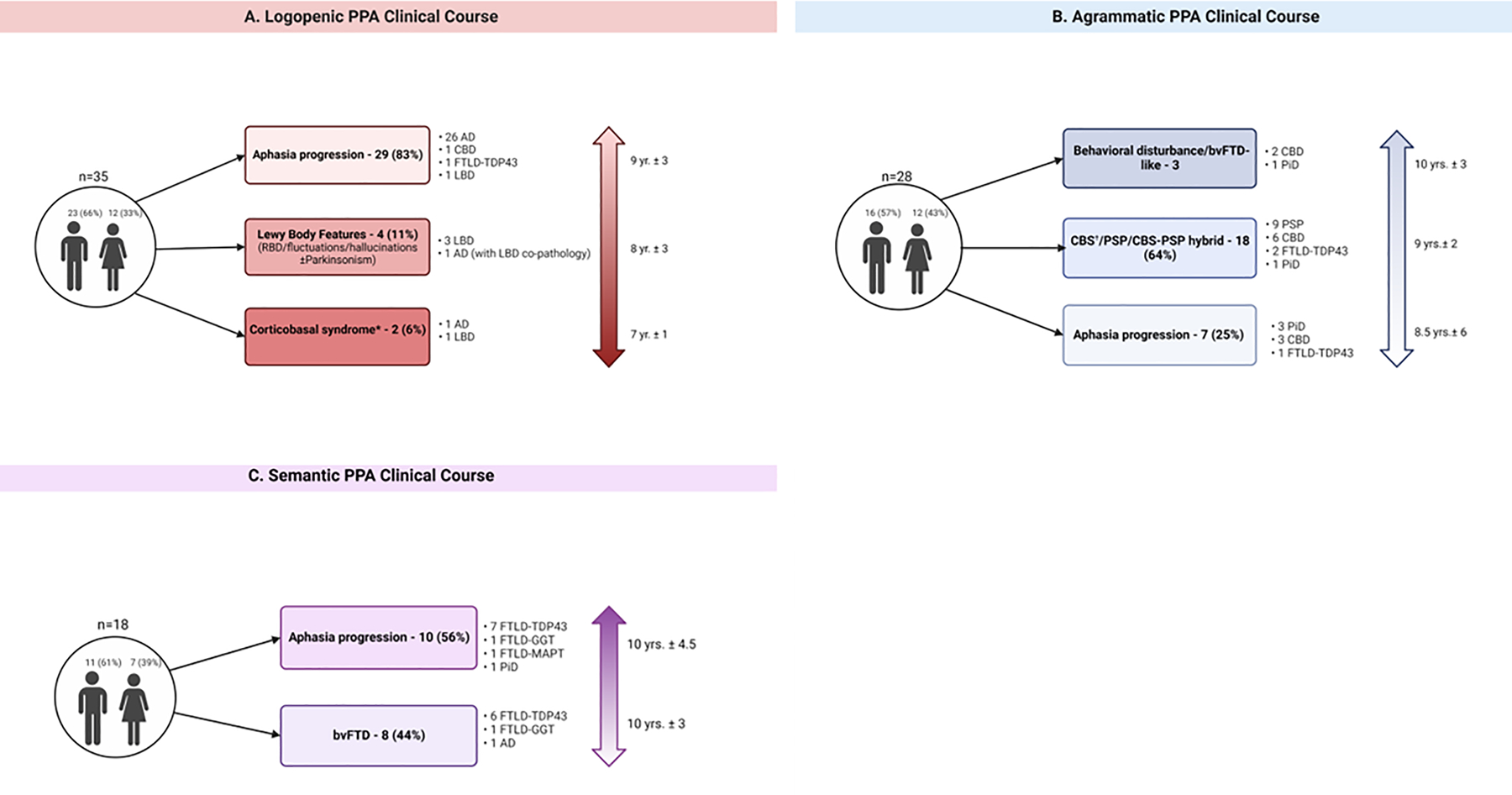
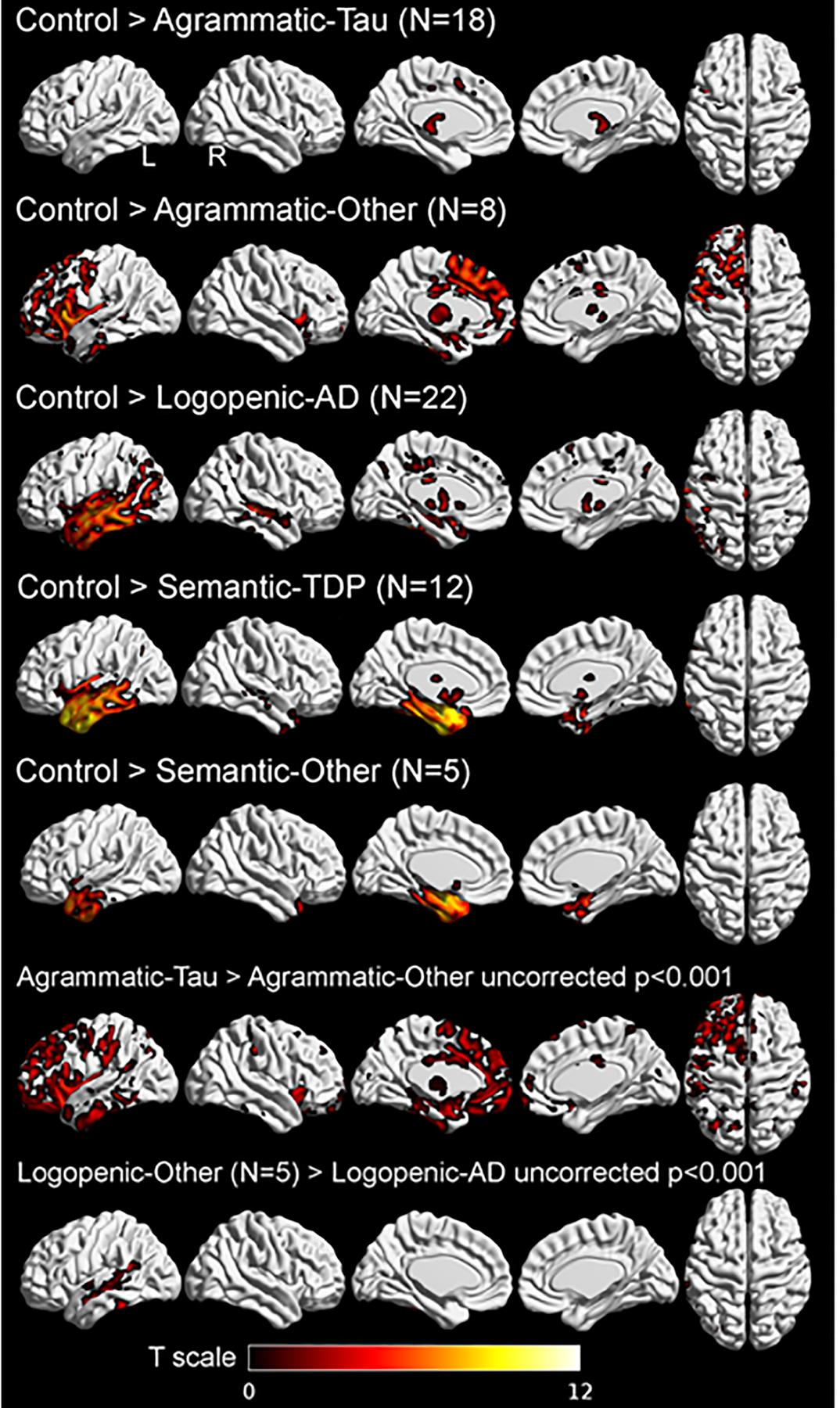
Results: PPA variant distribution: 35 lvPPA (80% AD), 28 agPPA (89% tauopathy) and 18 svPPA (72% frontotemporal lobar degeneration-TAR DNA-binding protein (FTLD-TDP)). Apraxia of speech was associated with 4R-tauopathy in agPPA, while pure agrammatic PPA without apraxia was linked to 3R-tauopathy. Longitudinal data revealed language dysfunction remained the predominant deficit for patients with lvPPA, agPPA evolved to corticobasal or progressive supranuclear palsy syndrome (64%) and svPPA progressed to behavioural variant frontotemporal dementia (44%). agPPA-4R-tauopathy exhibited limited pre-supplementary motor area atrophy, lvPPA-AD displayed temporal atrophy extending to the superior temporal sulcus and svPPA-FTLD-TDP had severe temporal pole atrophy. The FDG-PET-based machine learning algorithm accurately predicted clinical diagnoses and underlying pathologies.
Conclusions: Distinguishing 3R-taupathy and 4R-tauopathy in agPPA may rely on apraxia of speech presence. Additional linguistic and clinical features can aid neuropathology prediction. Our data-driven brain metabolism decomposition approach effectively predicts underlying neuropathology.
Keywords: APHASIA; MRI.
© Author(s) (or their employer(s)) 2024. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DSK serves on a Data Safety Monitoring Board for the DIAN study. He served on a Data Safety Monitoring Board for a tau therapeutic for Biogen but receives no personal compensation. He is a site investigator in the Biogen aducanumab trials. He is an investigator in a clinical trial sponsored by Lilly Pharmaceuticals and the University of Southern California. He serves as a consultant for Samus Therapeutics, Roche and Alzeca Biosciences but receives no personal compensation. RCP serves as a consultant for Roche, Genentech, Nestle, Eli Lilly and Co and Eisai, and receives publishing royalties from Mild Cognitive Impairment (Oxford University Press, 2003) and UpToDate. BFB receives honoraria for SAB activities for the Tau Consortium; is a site investigator for clinical trials sponsored by Alector, Biogen and Transposon; and receives research support from NIH. GSD serves as a consultant for Parabon NanoLabs, as a topic editor (Dementia) for DynaMed (EBSCO) and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation (Canada, uncompensated). He is the co-Project PI for a clinical trial in Anti-NMDA Receptor Encephalitis, which receives support from Horizon Pharmaceuticals. He has developed educational materials for PeerView Media and Continuing Education. He owns stock in ANI Pharmaceuticals. GSD’s institution has received support from Eli Lilly for GSD’s development and participation in an educational event promoting early diagnosis of symptomatic Alzheimer's disease. WKK was supported in part by NIH funding. DWD, DTJ, KAJ and JLW received research funding from the NIH and declared no competing financial interests. MEM is a consultant for AVID Radiopharmaceuticals. She receives support from the NIH/NIA and Eli Lilly. NRG-R receives royalties from UpToDate, has participated in multicentre therapy studies sponsored by Biogen, TauRx, AbbVie, Novartis and Lilly, and he receives research support from NIH. JAF is on the OSMB for the SWAN-Aging Study, serves as a consultant for Medtronic and received NIH funding. JG-R serves on the DSMB for STROKENET, is a site investigator for a trial sponsored by Eisai and the NIH, and he receives research support from the NIH.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical