

Technical note: preliminary surgical experience with a new implantable epicranial stimulation device for chronic focal cortex stimulation in drug-resistant epilepsy
- PMID: 38514531
- PMCID: PMC10957708
- DOI: 10.1007/s00701-024-06022-0
Technical note: preliminary surgical experience with a new implantable epicranial stimulation device for chronic focal cortex stimulation in drug-resistant epilepsy
Abstract
Purpose: This study is to report some preliminary surgical considerations and outcomes after the first implantations of a new and commercially available implantable epicranial stimulation device for focal epilepsy.
Methods: We retrospectively analyzed data from clinical notes. Outcome parameters were as follows: wound healing, surgery time, and adverse events.
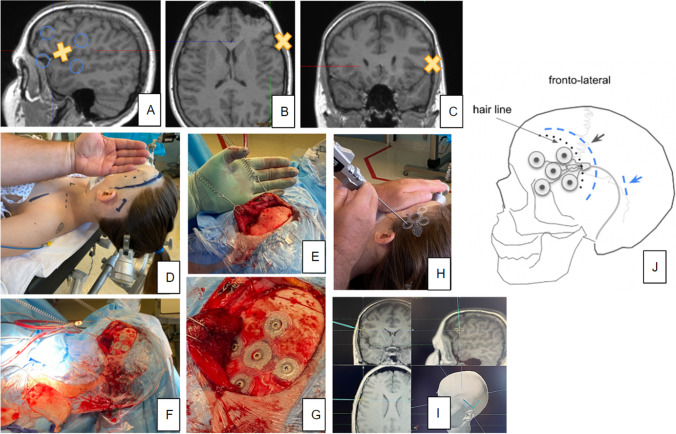
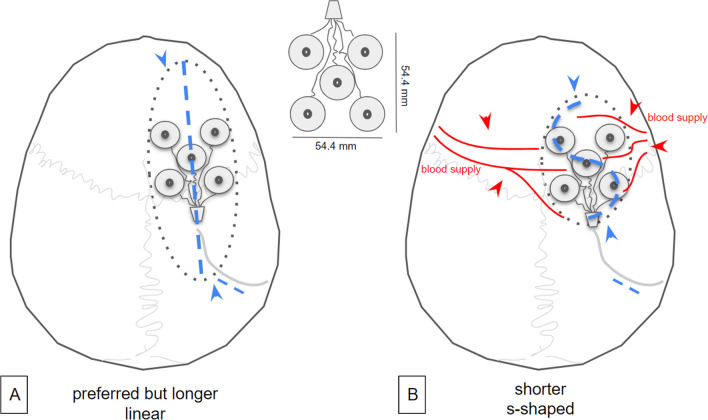
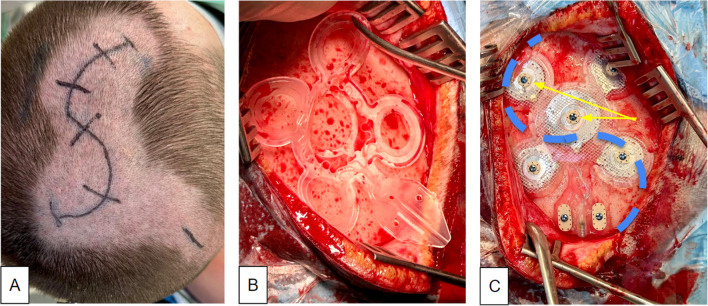
Results: Five patients were included (17-52 y/o; 3 female). Epicranial systems were uneventfully implanted under neuronavigation guidance. Some minor adverse events occurred. Wound healing in primary intention was seen in all patients. Out of these surgeries, certain concepts were developed: Skin incisions had to be significantly larger than expected. S-shaped incisions appeared to be a good choice in typical locations behind the hairline. Preoperative discussions between neurologist and neurosurgeon are mandatory in order to allow for the optimal coverage of the epileptogenic zone with the electrode geometry.
Conclusion: In this first small series, we were able to show safe implantation of this new epicranial stimulation device. The use of neuronavigation is strongly recommended. The procedure is simple but not trivial and ideally belongs in the hands of a neurosurgeon.
Keywords: Chronic epicranial focal cortex stimulation; Drug-resistant epilepsy; Neuromodulation; Surgical experience.
© 2024. The Author(s).
Conflict of interest statement
Unrelated: VAC receives an ongoing collaborative grant from BrainLab (Munich, Germany). He serves as an advisor for Ceregate (Munich, Germany), Cortec (Freiburg, Germany), and Inbrain (Barcelona, Spain). He has an ongoing IIT with Boston Scientific (USA). He has received travel support and personal honoraria for lecturing services from Boston Scientific (USA) and UNEEG Medical (Munich, Germany). ASB has received research support from BIAL and UNEEG and has received personal honoraria for lectures and advice from Angelini, BIAL, Desitin, Jazz pharma, UCB, and UNEEG. BEAS receives a research grant from Ceregate (Hamburg, Germany) unrelated to this publication. PCR receives research support from: Else Kröner-Fresenius Foundation (Germany) and Fraunhofer Foundation (Germany). He is a consultant for Boston Scientific (USA), Inomed (Germany), and Brainlab (Germany) and has received honoraria for lectures from Arkana, Germany. NJ, BKS, and MH have nothing to declare.
Related: VAC is a coordinating investigator (LKP) in the EASEE4YOU study (DRKS00031722) sponsored by Precisis, Heidelberg. He has received travel support and personal honoraria for lecturing services from Precisis (Heidelberg, Germany). ASB has received research support from PRECISIS and has received personal honoraria for lectures and advice from Precisis, Heidelberg. TB serves as an investigator in the EASEE4YOU study and has previously received honoraria by Precisis (Heidelberg, Germany) for advice.
Beyond the above mentioned, the authors do not have any commercial interest in the device described herein.
Figures

References
-
- Fisher R, Salanova V, Witt T et al (2010) Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory epilepsy. Epilepsia 51(5):899–908 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
