

Long-term risk of psychiatric disorder and psychotropic prescription after SARS-CoV-2 infection among UK general population
- PMID: 38514769
- PMCID: PMC11199144
- DOI: 10.1038/s41562-024-01853-4
Long-term risk of psychiatric disorder and psychotropic prescription after SARS-CoV-2 infection among UK general population
Abstract
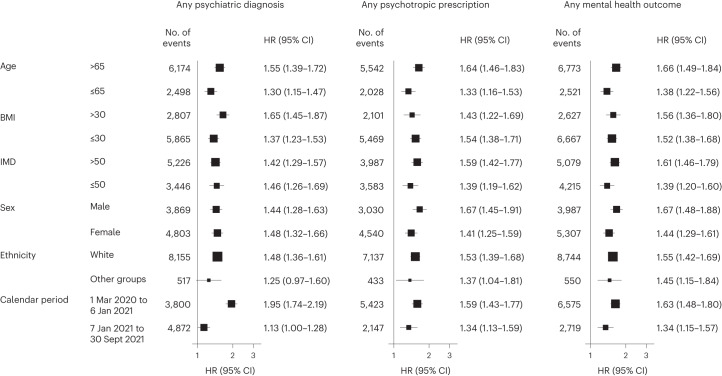
Despite evidence indicating increased risk of psychiatric issues among COVID-19 survivors, questions persist about long-term mental health outcomes and the protective effect of vaccination. Using UK Biobank data, three cohorts were constructed: SARS-CoV-2 infection (n = 26,101), contemporary control with no evidence of infection (n = 380,337) and historical control predating the pandemic (n = 390,621). Compared with contemporary controls, infected participants had higher subsequent risks of incident mental health at 1 year (hazard ratio (HR): 1.54, 95% CI 1.42-1.67; P = 1.70 × 10-24; difference in incidence rate: 27.36, 95% CI 21.16-34.10 per 1,000 person-years), including psychotic, mood, anxiety, alcohol use and sleep disorders, and prescriptions for antipsychotics, antidepressants, benzodiazepines, mood stabilizers and opioids. Risks were higher for hospitalized individuals (2.17, 1.70-2.78; P = 5.80 × 10-10) than those not hospitalized (1.41, 1.30-1.53; P = 1.46 × 10-16), and were reduced in fully vaccinated people (0.97, 0.80-1.19; P = 0.799) compared with non-vaccinated or partially vaccinated individuals (1.64, 1.49-1.79; P = 4.95 × 10-26). Breakthrough infections showed similar risk of psychiatric diagnosis (0.91, 0.78-1.07; P = 0.278) but increased prescription risk (1.42, 1.00-2.02; P = 0.053) compared with uninfected controls. Early identification and treatment of psychiatric disorders in COVID-19 survivors, especially those severely affected or unvaccinated, should be a priority in the management of long COVID. With the accumulation of breakthrough infections in the post-pandemic era, the findings highlight the need for continued optimization of strategies to foster resilience and prevent escalation of subclinical mental health symptoms to severe disorders.
© 2024. The Author(s).
Conflict of interest statement
C.G.-R. has received honoraria/travel support from Abbot, Angelini, Cassen-Recordati, Janssen-Cilag, and Lundbeck. D.P.-A. reported grants from Amgen, UCB Biopharma, Les Laboratoires Servier, Novartis, and Chiesi-Taylor, as well as speaker fees and advisory board membership with AstraZeneca and Johnson and Johnson outside the submitted work, in addition to research support from Janssen. The remaining authors declare no competing interests.
Figures





References
-
- WHO COVID-19 Dashboard (World Health Organization, 2024).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
