

Clustering COVID-19 ARDS patients through the first days of ICU admission. An analysis of the CIBERESUCICOVID Cohort
- PMID: 38515193
- PMCID: PMC10958830
- DOI: 10.1186/s13054-024-04876-5
Clustering COVID-19 ARDS patients through the first days of ICU admission. An analysis of the CIBERESUCICOVID Cohort
Abstract
Background: Acute respiratory distress syndrome (ARDS) can be classified into sub-phenotypes according to different inflammatory/clinical status. Prognostic enrichment was achieved by grouping patients into hypoinflammatory or hyperinflammatory sub-phenotypes, even though the time of analysis may change the classification according to treatment response or disease evolution. We aimed to evaluate when patients can be clustered in more than 1 group, and how they may change the clustering of patients using data of baseline or day 3, and the prognosis of patients according to their evolution by changing or not the cluster.
Methods: Multicenter, observational prospective, and retrospective study of patients admitted due to ARDS related to COVID-19 infection in Spain. Patients were grouped according to a clustering mixed-type data algorithm (k-prototypes) using continuous and categorical readily available variables at baseline and day 3.
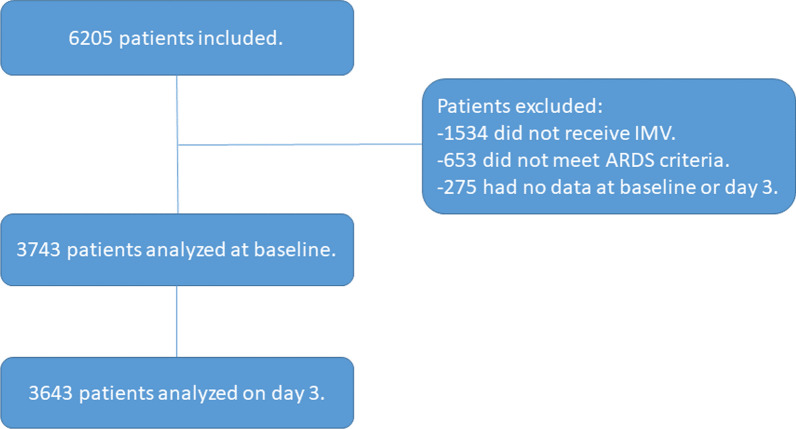
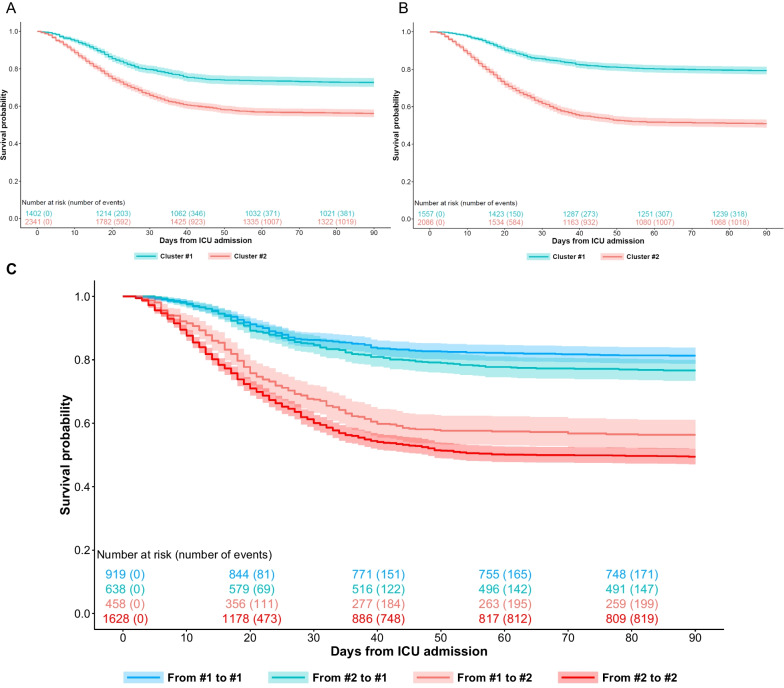
Results: Of 6205 patients, 3743 (60%) were included in the study. According to silhouette analysis, patients were grouped in two clusters. At baseline, 1402 (37%) patients were included in cluster 1 and 2341(63%) in cluster 2. On day 3, 1557(42%) patients were included in cluster 1 and 2086 (57%) in cluster 2. The patients included in cluster 2 were older and more frequently hypertensive and had a higher prevalence of shock, organ dysfunction, inflammatory biomarkers, and worst respiratory indexes at both time points. The 90-day mortality was higher in cluster 2 at both clustering processes (43.8% [n = 1025] versus 27.3% [n = 383] at baseline, and 49% [n = 1023] versus 20.6% [n = 321] on day 3). Four hundred and fifty-eight (33%) patients clustered in the first group were clustered in the second group on day 3. In contrast, 638 (27%) patients clustered in the second group were clustered in the first group on day 3.
Conclusions: During the first days, patients can be clustered into two groups and the process of clustering patients may change as they continue to evolve. This means that despite a vast majority of patients remaining in the same cluster, a minority reaching 33% of patients analyzed may be re-categorized into different clusters based on their progress. Such changes can significantly impact their prognosis.
Keywords: ARDS; Clustering; Mortality; Precision medicine.
© 2024. The Author(s).
Conflict of interest statement
Dr. Roca reported a research grant from Hamilton Medical AG and Fisher & Paykel Healthcare Ltd., speaker fees from Hamilton Medical AG, Fisher & Paykel Healthcare Ltd., and Aerogen Ltd., and non-financial research support from Timpel; all outside the submitted work. Minority stakeholder of Tesai Care SL, a spin-off of Parc Taulí University Hospital. The other authors have no conflict of interest to report.
Figures


References
-
- Acute Respiratory Distress Syndrome Network; Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
