

Middle meningeal artery embolization for the treatment of unilateral large chronic subdural hematoma patients with significant midline shift: A single-center experience
- PMID: 38515352
- PMCID: PMC11571913
- DOI: 10.1177/15910199241239706
Middle meningeal artery embolization for the treatment of unilateral large chronic subdural hematoma patients with significant midline shift: A single-center experience
Abstract
Background: The amount of midline shift (MLS) considered safe for middle meningeal artery embolization (MMAE) in patients with chronic subdural hematoma (CSDH) has not been established. Whether MMAE could be used as upfront treatment for unilateral large CSDH patients with significant MLS (>1 cm) has not been reported.
Objective: To investigate the efficacy and safety of MMAE in unilateral large CSDH patients with MLS > 1 cm.
Methods: Eleven carefully selected CSDH patients with mild or moderate symptoms and significant MLS > 1 cm from 1 May 2021 to 31 August 2022 were included in the study. All patients were treated with MMAE using polyvinyl alcohol (PVA) particles. Outcomes were assessed clinically and with interval imaging studies at follow-up.
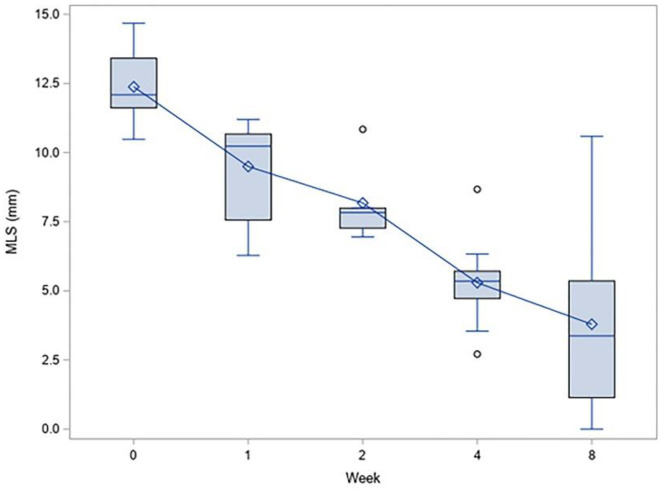
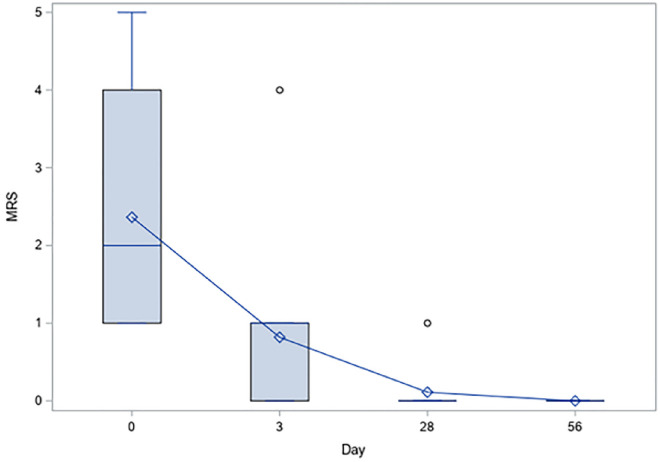
Results: All 19 MMAs (unilateral embolization in three patients and bilateral embolization in eight patients) were successfully embolized. All 11 patients were followed for subsequent months, and there was no recurrence and enlargement of CSDH. Procedural adverse events, mortality, or complications were not observed. The average time to achieve a 50% reduction in MLS was approximately four weeks, while it took approximately eight weeks to achieve a 50% reduction in maximal volume. All 11 patients showed improvement in their neurological symptoms at three days post-operation, including four hemiplegic patients.
Conclusions: MMAE may demonstrate safety in carefully selected CSDH patients with significant midline shift (MLS > 1 cm), particularly in those who are not suitable for surgery, thus providing a potential alternative approach.
Keywords: 3D-TOF MRA; Chronic subdural hematoma; interventional embolization; middle meningeal artery; midline shift.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Ivamoto HS, Lemos Jr HP, Atallah AN. Surgical treatments for chronic subdural hematomas: a comprehensive systematic review. World Neurosurg 2016; 86: 399–418. - PubMed
-
- Almenawer SA, Farrokhyar F, Hong C, et al. Chronic subdural hematoma management: a systematic review and meta-analysis of 34,829 patients. Ann Surg 2014; 259: 449–457. - PubMed
-
- Kolias AG, Chari A, Santarius T, et al. Chronic subdural haematoma: modern management and emerging therapies. Nat Rev Neurol 2014; 10: 570–578. - PubMed
-
- Adusumilli G, Ghozy S, Kallmes KM, et al. Common data elements reported on middle meningeal artery embolization in chronic subdural hematoma: an interactive systematic review of recent trials. J Neurointerv Surg 2022; 14: 1027–1032. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
