

Assessment of Frequency and Predictive Value of Comorbidities in Patients With Disorders of Consciousness in the Acute Setting
- PMID: 38515549
- PMCID: PMC10956526
- DOI: 10.1089/neur.2023.0120
Assessment of Frequency and Predictive Value of Comorbidities in Patients With Disorders of Consciousness in the Acute Setting
Abstract
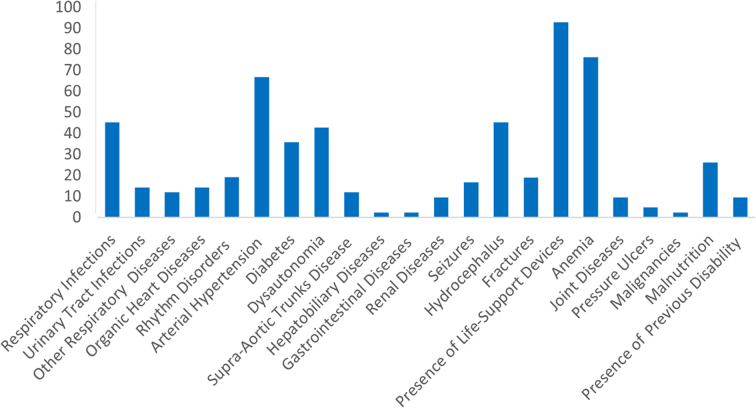
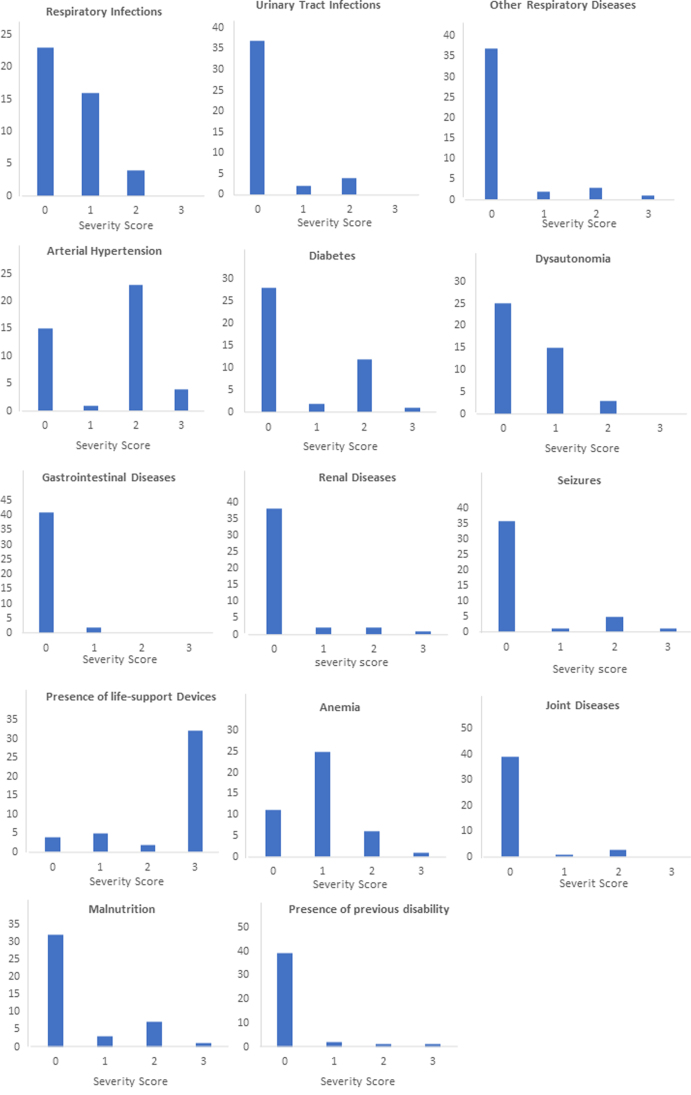
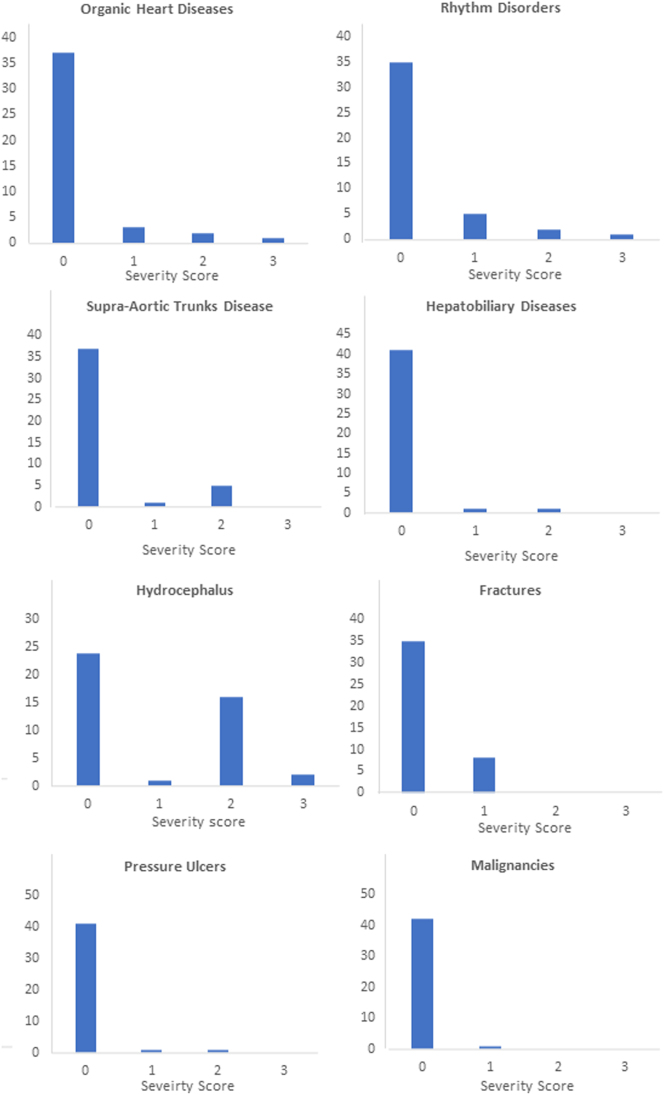
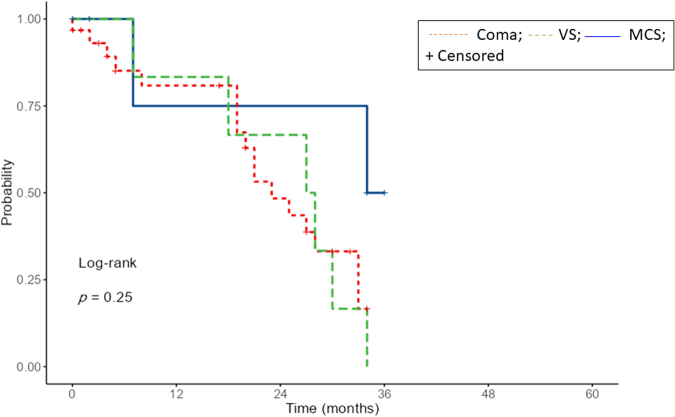
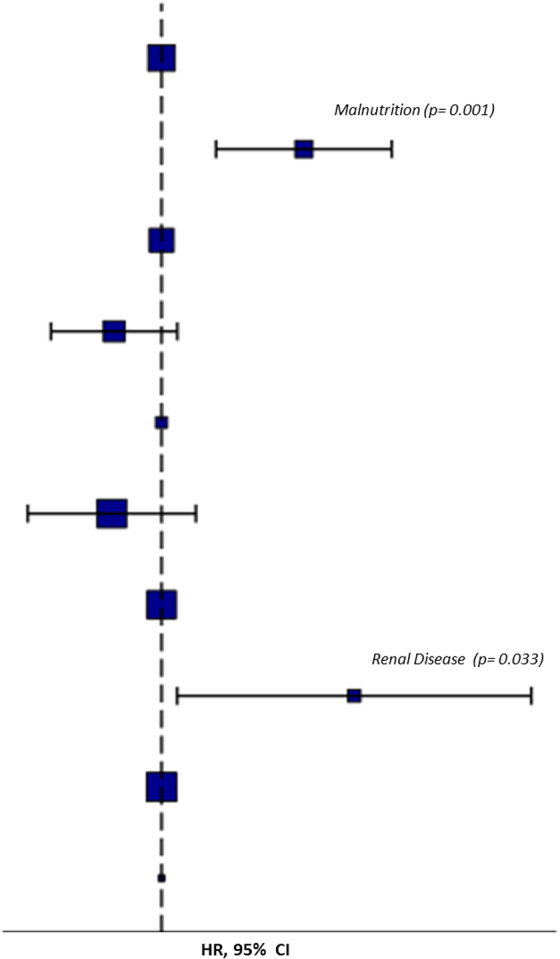
Medical comorbidities are frequent in patients with disorders of consciousness (DoC) and their impact on outcomes is under investigation. The aim of this study was to investigate patients with DoC in the acute stage and the influence of comorbidities. Patients admitted to intensive care units and neurological units with a diagnosis of coma, vegetative state/unresponsive wakefulness syndrome (VS/UWS), and minimally conscious state (MCS) were investigated through the Glasgow Coma Scale (GCS), the Coma Recovery Scale - Revised (CRS-R) and the Comorbidities Coma Scale (CoCos). Forty-three patients (21 men and 22 women; mean age at admission: 60.4 ± 21.0) were included in the study. The most frequent diagnosis at admission was coma (72%) followed by VS/UWS (14%) and MCS (14%). The most frequent brain injury was subarachnoid hemorrhage (46%). At the 6-month follow-up, 19 patients had died (44%), 15 showed a full recovery of consciousness (35%), 7 were in a condition of emergence from MCS (16%), and 2 showed a persistent VS/UWS (5%). Forty-two (98%) patients showed at least one comorbidity: presence of life-support device (92.9%), anemia (76.2%), arterial hypertension (66,7%), hydrocephalus (45.3%), and respiratory infections (45.2%) were those most frequently reported. At the Multivariable Cox regression, the presence of renal disease (hazard ratio [HR] 33.37; p = 0.033) and malnutrition (HR 14.52; p = 0.001) were predictors of missed recovery of full consciousness. Although adverse outcomes are generally predicted by the severity of brain damage, the presence of medical comorbidities in an acute phase could influence outcomes and long-term prognosis.
Keywords: CoCos; coma; comorbidities; minimally conscious state; vegetative state (unresponsive wakefulness syndrome).
© Gennaro Saporito et al., 2024; Published by Mary Ann Liebert, Inc.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
Recovery from prolonged disorders of consciousness: A dual-center prospective cohort study in China.World J Clin Cases. 2020 Jun 26;8(12):2520-2529. doi: 10.12998/wjcc.v8.i12.2520. World J Clin Cases. 2020. PMID: 32607329 Free PMC article.
-
Neck muscle spasticity in patients with disorder of consciousness: a pilot study.Eur J Phys Rehabil Med. 2024 Jun;60(3):412-419. doi: 10.23736/S1973-9087.24.08176-0. Epub 2024 Mar 19. Eur J Phys Rehabil Med. 2024. PMID: 38502553 Free PMC article.
-
Behavioral scales variability in patients with prolonged disorders of consciousness.Neurol Sci. 2023 Sep;44(9):3107-3122. doi: 10.1007/s10072-023-06812-x. Epub 2023 Apr 22. Neurol Sci. 2023. PMID: 37087504 Free PMC article.
-
Medical comorbidities in patients with prolonged disorder of consciousness: A narrative review.NeuroRehabilitation. 2024;54(1):61-73. doi: 10.3233/NRE-230130. NeuroRehabilitation. 2024. PMID: 38217620 Review.
-
EEG-based Brain-Computer Interfaces for people with Disorders of Consciousness: Features and applications. A systematic review.Front Hum Neurosci. 2022 Dec 5;16:1040816. doi: 10.3389/fnhum.2022.1040816. eCollection 2022. Front Hum Neurosci. 2022. PMID: 36545350 Free PMC article.
References
-
- Plum F, Posner JB. The diagnosis of stupor and coma. Contemp Neurol Ser 1972;10:1–286. - PubMed
LinkOut - more resources
Full Text Sources