

Longitudinal changes in medial meniscus extrusion and clinical outcomes following pullout repair for medial meniscus posterior root tears: a 3-year evaluation
- PMID: 38517526
- PMCID: PMC11101586
- DOI: 10.1007/s00590-024-03889-8
Longitudinal changes in medial meniscus extrusion and clinical outcomes following pullout repair for medial meniscus posterior root tears: a 3-year evaluation
Abstract
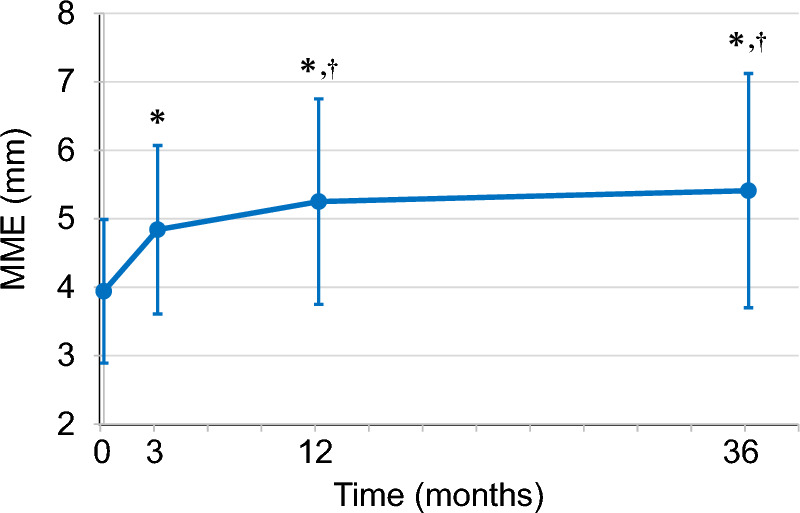
Purpose: We aimed to evaluate the longitudinal changes in medial meniscus extrusion (MME) and clinical scores at multiple time points up to 3 years after pullout repair for medial meniscus posterior root tears (MMPRTs).
Methods: This retrospective case series study included 64 patients who underwent pullout repair for MMPRTs and four MRI evaluations (preoperatively and at 3 months, 1 year, and 3 years postoperatively). MME was measured during the same time points. Clinical scores were assessed four times: preoperatively and at 1, 2, and 3 years postoperatively. Additionally, a multivariate analysis was performed on the change in MME (ΔMME) from the preoperative measurement point to 3 years postoperatively.
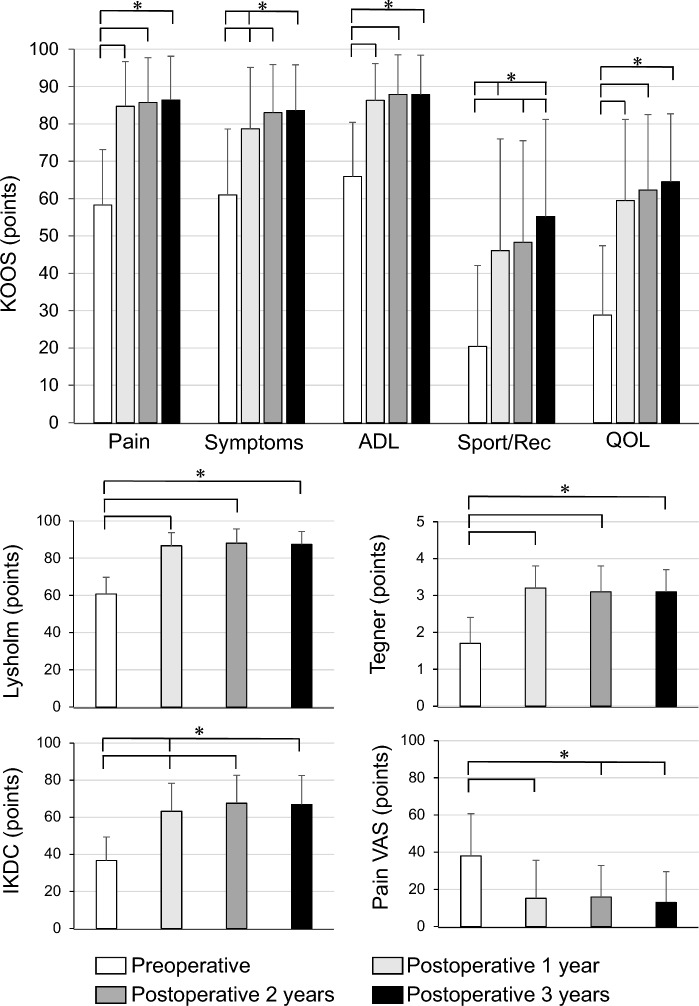
Results: The ΔMME per month from the preoperative measurement point to 3 months postoperatively, from 3 months to 1 year postoperatively, and from 1 to 3 years postoperatively were 0.30, 0.05, and 0.01 mm/month, respectively. All clinical scores significantly improved 3 years postoperatively (p < 0.001). In a multiple regression analysis for ΔMME from the preoperative measurement point to 3 years postoperatively, sex significantly affected the outcome (p = 0.039).
Conclusion: Following pullout repair for MMPRTs with well-aligned lower extremities, although MME progression could not be entirely prevented, the rate of progression decreased over time, and clinical scores improved. In particular, MME progressed markedly during the first 3 months postoperatively. Additionally, sex had a significant influence on MME progression, suggesting that males may be able to expand the indications of pullout repair for MMPRTs.
Keywords: Clinical score; Meniscus; Meniscus extrusion; Osteoarthritis; Posterior root tear.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
Similar articles
-
Signal intensity of repaired posterior roots after transtibial pullout repair for medial meniscus posterior root tears in stable knees: Magnetic resonance imaging evaluations at 3 years postoperatively.Knee. 2024 Jun;48:22-29. doi: 10.1016/j.knee.2024.02.014. Epub 2024 Mar 14. Knee. 2024. PMID: 38484441
-
Meniscal healing status after medial meniscus posterior root repair negatively correlates with a midterm increase in medial meniscus extrusion.Knee Surg Sports Traumatol Arthrosc. 2024 Sep;32(9):2219-2227. doi: 10.1002/ksa.12245. Epub 2024 May 13. Knee Surg Sports Traumatol Arthrosc. 2024. PMID: 38741370
-
Weight loss enhances meniscal healing following transtibial pullout repair for medial meniscus posterior root tears.Knee Surg Sports Traumatol Arthrosc. 2024 Jan;32(1):143-150. doi: 10.1002/ksa.12037. Epub 2024 Jan 4. Knee Surg Sports Traumatol Arthrosc. 2024. PMID: 38226719
-
The Early Arthroscopic Pullout Repair of Medial Meniscus Posterior Root Tear Is More Effective for Reducing Medial Meniscus Extrusion.Acta Med Okayama. 2019 Dec;73(6):503-510. doi: 10.18926/AMO/57714. Acta Med Okayama. 2019. PMID: 31871332
-
Comparison of Long-term Radiographic Outcomes and Rate and Time for Conversion to Total Knee Arthroplasty Between Repair and Meniscectomy for Medial Meniscus Posterior Root Tears: A Systematic Review and Meta-analysis.Am J Sports Med. 2022 Jun;50(7):2023-2031. doi: 10.1177/03635465211017514. Epub 2021 Jul 12. Am J Sports Med. 2022. PMID: 34251898
Cited by
-
Biomechanical comparison of all-inside meniscal suture configurations for posterior root tear: Three conventional stitches versus delta-grip stitch.J Exp Orthop. 2025 Jan 22;12(1):e70149. doi: 10.1002/jeo2.70149. eCollection 2025 Jan. J Exp Orthop. 2025. PMID: 39845700 Free PMC article.
-
Quadriceps muscle strength of the affected limb in medial meniscus posterior root tears is negatively correlated with the progression of postoperative medial joint space narrowing.J Exp Orthop. 2024 Dec 12;11(4):e70057. doi: 10.1002/jeo2.70057. eCollection 2024 Oct. J Exp Orthop. 2024. PMID: 39678022 Free PMC article.
-
The use of lateral wedge insoles delays osteoarthritis progression and improves clinical outcomes in medial meniscus posterior root repair.J Exp Orthop. 2025 Jan 20;12(1):e70141. doi: 10.1002/jeo2.70141. eCollection 2025 Jan. J Exp Orthop. 2025. PMID: 39839858 Free PMC article.
-
Arthroscopic Knotless Anchor Through High Posterolateral Portal for Treating Medial Meniscal Posterior Root Tears.Arthrosc Tech. 2025 Feb 10;14(5):103457. doi: 10.1016/j.eats.2025.103457. eCollection 2025 May. Arthrosc Tech. 2025. PMID: 40547976 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
