

Racial and ethnic associations with comprehensive cancer center access and clinical trial enrollment for acute leukemia
- PMID: 38518098
- PMCID: PMC11223832
- DOI: 10.1093/jnci/djae067
Racial and ethnic associations with comprehensive cancer center access and clinical trial enrollment for acute leukemia
Abstract
Background: Clinical trial participation at Comprehensive Cancer Centers (CCC) is inequitable for minoritized racial and ethnic groups with acute leukemia. CCCs care for a high proportion of adults with acute leukemia. It is unclear if participation inequities are due to CCC access, post-access enrollment, or both.
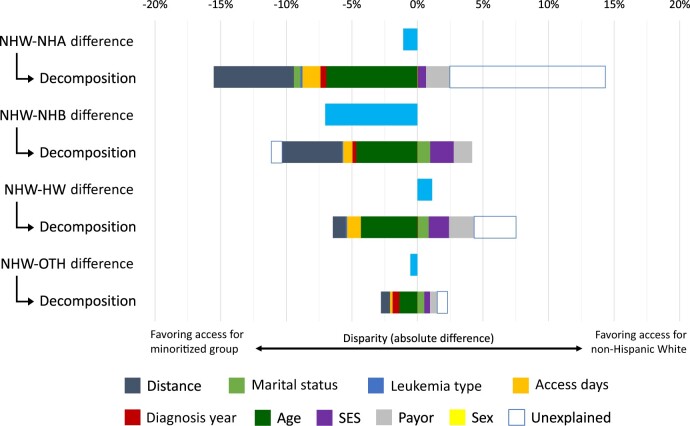
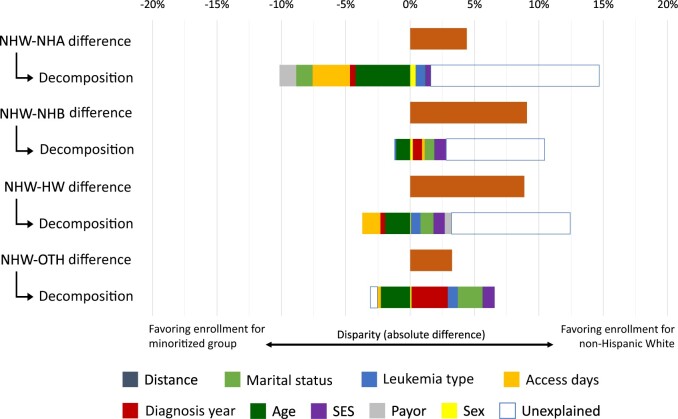
Methods: We conducted a retrospective cohort study of adults with acute leukemia (2010-2019) residing within Massachusetts, the designated catchment area of the Dana-Farber/Harvard Cancer Center (DF/HCC). Individuals were categorized as non-Hispanic Asian (NHA), Black (NHB), White (NHW), Hispanic White (HW), or Other. Decomposition analyses assessed covariate contributions to disparities in (1) access to DF/HCC care and (2) post-access enrollment.
Results: Of 3698 individuals with acute leukemia, 85.9% were NHW, 4.5% HW, 4.3% NHB, 3.7% NHA, and 1.3% Other. Access was lower for HW (age- and sex-adjusted OR = 0.64, 95% CI = 0.45 to 0.90) and reduced post-access enrollment for HW (aOR = 0.54, 95% CI =0.34 to 0.86) and NHB (aOR = 0.60, 95% CI = 0.39 to 0.92) compared to NHW. Payor and socioeconomic status (SES) accounted for 25.2% and 21.2% of the +1.1% absolute difference in HW access. Marital status and SES accounted for 8.0% and 7.0% of the -8.8% absolute disparity in HW enrollment; 76.4% of the disparity was unexplained. SES and marital status accounted for 8.2% and 7.1% of the -9.1% absolute disparity in NHB enrollment; 73.0% of the disparity was unexplained.
Conclusions: A substantial proportion of racial and ethnic inequities in acute leukemia trial enrollment at CCCs are from post-access enrollment, the majority of which was not explained by sociodemographic factors.
© The Author(s) 2024. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
Dr Hantel reports receiving personal fees (advisory boards) from AstraZeneca and AbbVie outside the submitted work. Dr Brunner receiving personal fees (consulting) from Agios, Acceleron, BMS/Celgene, Gilead, Keros Therapeutics, Novartis, and Takeda and BMS (advisory board) outside the submitted work. Dr Varela reports receiving personal fees (speakers bureau) from Gilead outside the submitted work and having stock options in NexImmune. Dr Luskin reports receiving personal fees (advisory boards) from Novartis and AbbVie outside the submitted work. Dr Stone reports receiving personal fees (consulting, advisory boards, steering committees, and/or data safety monitoring board participation) for GSK, Hermavant, Takeda, AMGEN, Aptevo, AvenCell, BerGenBio, Cellularity, CTI Pharma, Epizyme, Jazz, Kura Onc, Rigel, and Syntrix outside the submitted work. Dr Lathan reports receiving personal fees (advisory boards) from BMS outside the submitted work. Dr DeAngelo reports receiving research funding from Abbvie, Novartis, Blueprint, and Glycomimetrics and personal fees (consulting) from Amgen, Autolus, Blueprint, Gilead, Incyte, Jazz, Kite, Novartis, Pfizer, Servier, and Takeda outside the submitted work. Dr Abel reports receiving personal fees (consultancy) from Novartis and Geron outside of the submitted work.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
