

Clinical drug screening reveals clofazimine potentiates the efficacy while reducing the toxicity of anti-PD-1 and CTLA-4 immunotherapy
- PMID: 38518774
- PMCID: PMC11756590
- DOI: 10.1016/j.ccell.2024.03.001
Clinical drug screening reveals clofazimine potentiates the efficacy while reducing the toxicity of anti-PD-1 and CTLA-4 immunotherapy
Abstract
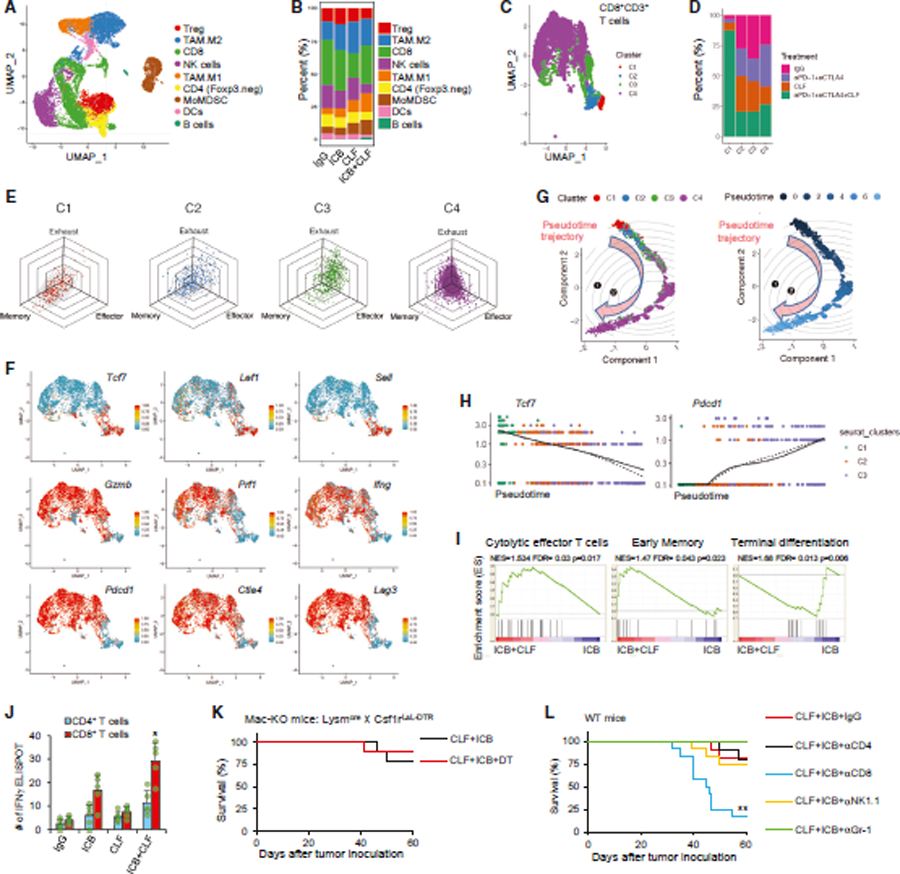
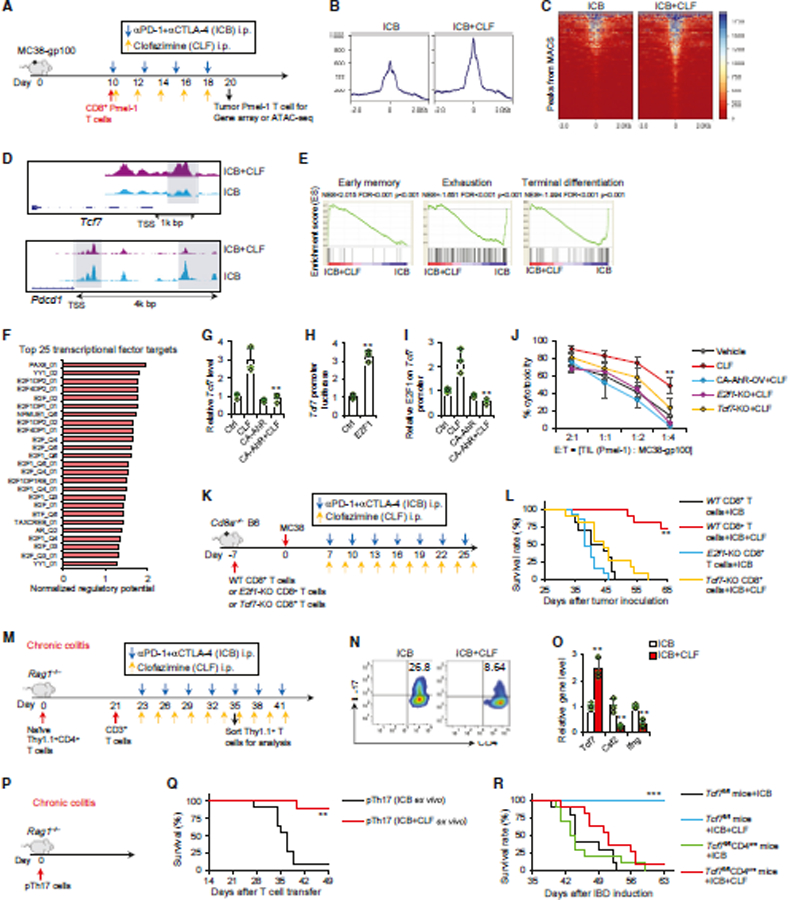
Emerging as the most potent and durable combinational immunotherapy, dual anti-PD-1 and CTLA-4 immune checkpoint blockade (ICB) therapy notoriously increases grade 3-5 immune-related adverse events (irAEs) in patients. Accordingly, attempts to improve the antitumor potency of anti-PD-1+CTLA-4 ICB by including additional therapeutics have been largely discouraged due to concerns of further increasing fatal toxicity. Here, we screened ∼3,000 Food and Drug Administration (FDA)-approved drugs and identified clofazimine as a potential third agent to optimize anti-PD-1+CTLA-4 ICB. Remarkably, clofazimine outperforms ICB dose reduction or steroid treatment in reversing lethality of irAEs, but unlike the detrimental effect of steroids on antitumor efficacy, clofazimine potentiates curative responses in anti-PD-1+CTLA-4 ICB. Mechanistically, clofazimine promotes E2F1 activation in CD8+ T cells to overcome resistance and counteracts pathogenic Th17 cells to abolish irAEs. Collectively, clofazimine potentiates the antitumor efficacy of anti-PD-1+CTLA-4 ICB, curbs intractable irAEs, and may fill a desperate clinical need to improve patient survival.
Copyright © 2024 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing financial interests.
Figures





References
-
- Vellanki PJ, Mulkey F, Jaigirdar AA, Rodriguez L, Xu Y, Zhao H, Liu J, Howe G, Wang J, et al. (2021). FDA approval summary: Nivolumab with ipilimumab and chemotherapy for metastatic non–small cell lung cancer, A collaborative project orbis review. Clin. Cancer Res 27, 3522–3527. 10.1158/1078-0432.CCR-20-4338. - DOI - PMC - PubMed
-
- Saung MT, Pelosof L, Casak S, Donoghue M, Lemery S, Yuan M, Rodriguez L, Schotland P, Chuk M, Davis G, et al. (2021). FDA Approval Summary: Nivolumab Plus Ipilimumab for the Treatment of Patients with Hepatocellular Carcinoma Previously Treated with Sorafenib. Oncologist 26, 797–806. 10.1002/onco.13819. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
