

Targeting refractory/recurrent neuroblastoma and osteosarcoma with anti-CD3×anti-GD2 bispecific antibody armed T cells
- PMID: 38519053
- PMCID: PMC10961524
- DOI: 10.1136/jitc-2023-008744
Targeting refractory/recurrent neuroblastoma and osteosarcoma with anti-CD3×anti-GD2 bispecific antibody armed T cells
Abstract
Background: The survival benefit observed in children with neuroblastoma (NB) and minimal residual disease who received treatment with anti-GD2 monoclonal antibodies prompted our investigation into the safety and potential clinical benefits of anti-CD3×anti-GD2 bispecific antibody (GD2Bi) armed T cells (GD2BATs). Preclinical studies demonstrated the high cytotoxicity of GD2BATs against GD2+cell lines, leading to the initiation of a phase I/II study in recurrent/refractory patients.
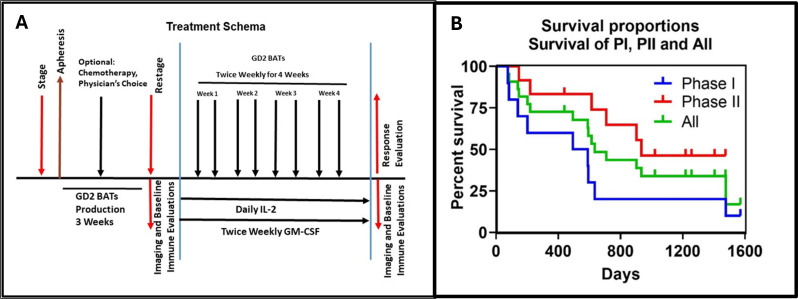
Methods: The 3+3 dose escalation phase I study (NCT02173093) encompassed nine evaluable patients with NB (n=5), osteosarcoma (n=3), and desmoplastic small round cell tumors (n=1). Patients received twice-weekly infusions of GD2BATs at 40, 80, or 160×106 GD2BATs/kg/infusion complemented by daily interleukin-2 (300,000 IU/m2) and twice-weekly granulocyte macrophage colony-stimulating factor (250 µg/m2). The phase II segment focused on patients with NB at the dose 3 level of 160×106 GD2BATs/kg/infusion.
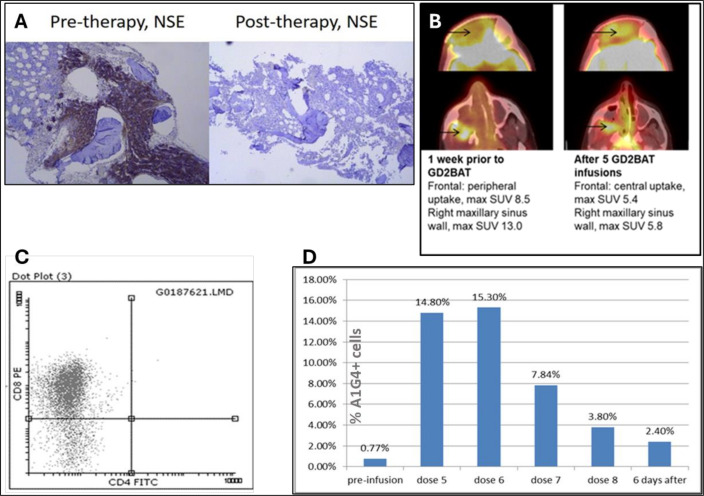
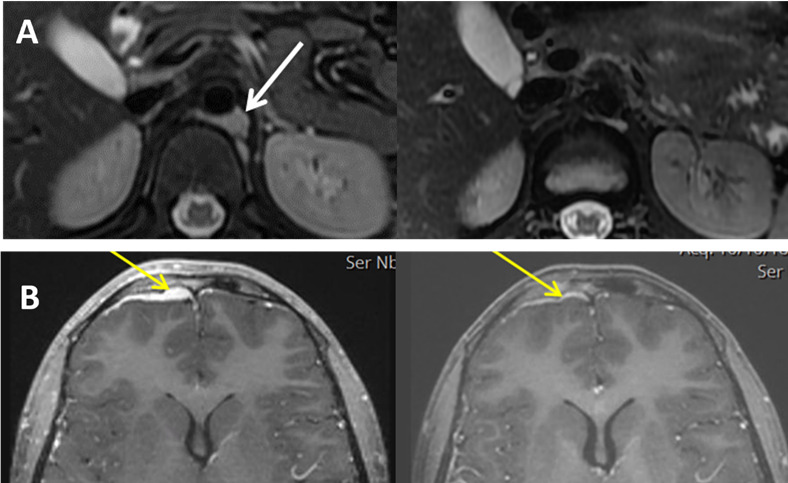
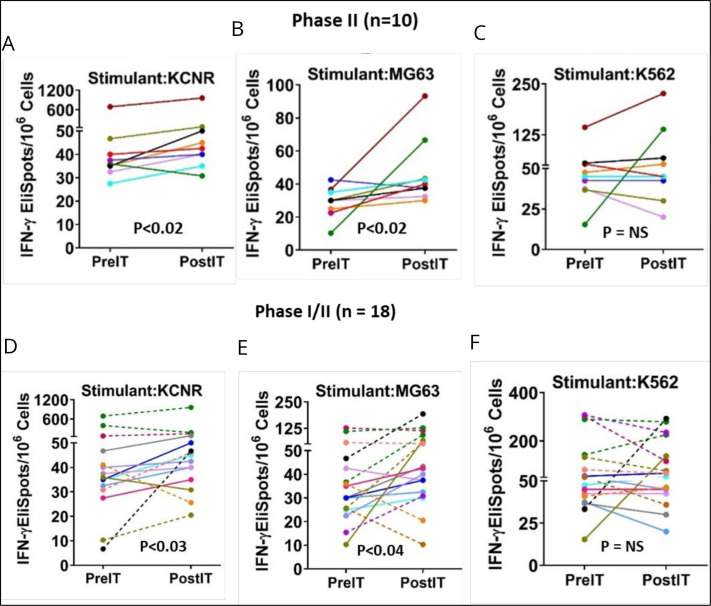
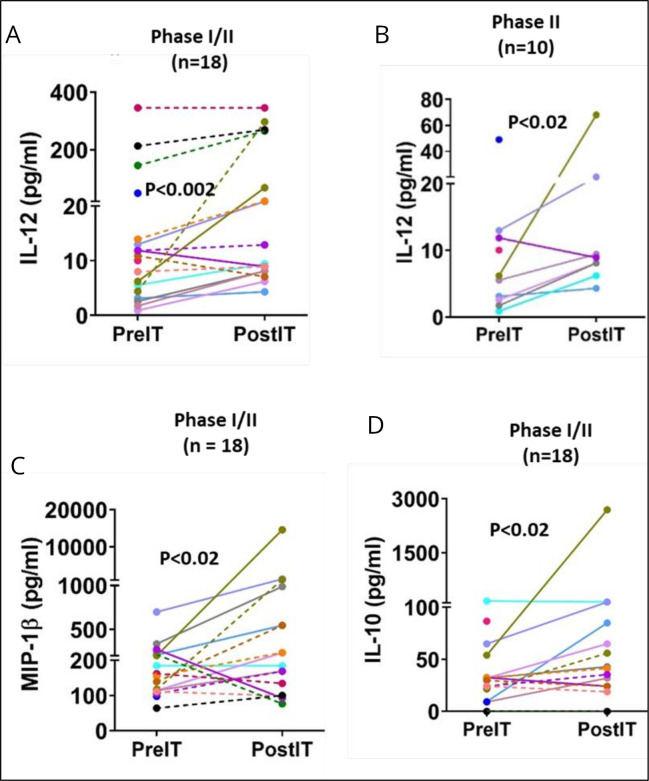
Results: Of the 12 patients enrolled, 9 completed therapy in phase I with no dose-limiting toxicities. Mild and manageable cytokine release syndrome occurred in all patients, presenting as grade 2-3 fevers/chills, headaches, and occasional hypotension up to 72 hours after GD2BAT infusions. GD2-antibody-associated pain was minimal. Median overall survival (OS) for phase I and the limited phase II was 18.0 and 31.2 months, respectively, with a combined OS of 21.1 months. A phase I NB patient had a complete bone marrow response with overall stable disease. In phase II, 10 of 12 patients were evaluable: 1 achieved partial response, and 3 showed clinical benefit with prolonged stable disease. Over 50% of evaluable patients exhibited augmented immune responses to GD2+targets post-GD2BATs, as indicated by interferon-gamma (IFN-γ) EliSpots, Th1 cytokines, and/or chemokines.
Conclusions: This study demonstrated the safety of GD2BATs up to 160×106 cells/kg/infusion. Coupled with evidence of post-treatment endogenous immune responses, our findings support further investigation of GD2BATs in larger phase II clinical trials.
Keywords: Adoptive cell therapy - ACT; Neuroblastoma.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LGL is co-founder of Transtarget and is a SAB member for Rapa Therapeutics. LGL is founder of BATs, LLC. LGL and AT were named as inventors in multiple patents filed by UV. Both MSK and N-KVC have financial interest in Y-mAbs, Abpro-Labs and Eureka Therapeutics. N-KVC reports receiving commercial research grants from Y-mabs Therapeutics and Abpro-Labs. N-KVC was named as inventor on multiple patents filed by MSK, including those licensed to Ymabs Therapeutics, Biotec Pharmacon, and Abpro-labs. N-KVC is a SAB member for Abpro-Labs and Eureka Therapeutics. AT is co-founder of Novo-Immune. DWL holds a CAR-T related patent and his university receives clinical trial funding from KITE Pharma/Gilead.
Figures
Update of
-
Targeting GD2-positive Refractory/Resistant Neuroblastoma and Osteosarcoma with Anti- CD3 x Anti-GD2 Bispecific Antibody Armed T cells.Res Sq [Preprint]. 2023 Nov 9:rs.3.rs-3570311. doi: 10.21203/rs.3.rs-3570311/v1. Res Sq. 2023. Update in: J Immunother Cancer. 2024 Mar 21;12(3):e008744. doi: 10.1136/jitc-2023-008744. PMID: 37986911 Free PMC article. Updated. Preprint.
References
-
- Berthold F, Ernst A, Hero B, et al. Long-term outcomes of the GPOH Nb97 trial for children with high-risk neuroblastoma comparing high-dose chemotherapy with autologous stem cell transplantation and oral chemotherapy as consolidation. Br J Cancer 2018;119:282–90. 10.1038/s41416-018-0169-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical