

Targeting pediatric cancers via T-cell recognition of the monomorphic MHC class I-related protein MR1
- PMID: 38519054
- PMCID: PMC10961533
- DOI: 10.1136/jitc-2023-007538
Targeting pediatric cancers via T-cell recognition of the monomorphic MHC class I-related protein MR1
Abstract
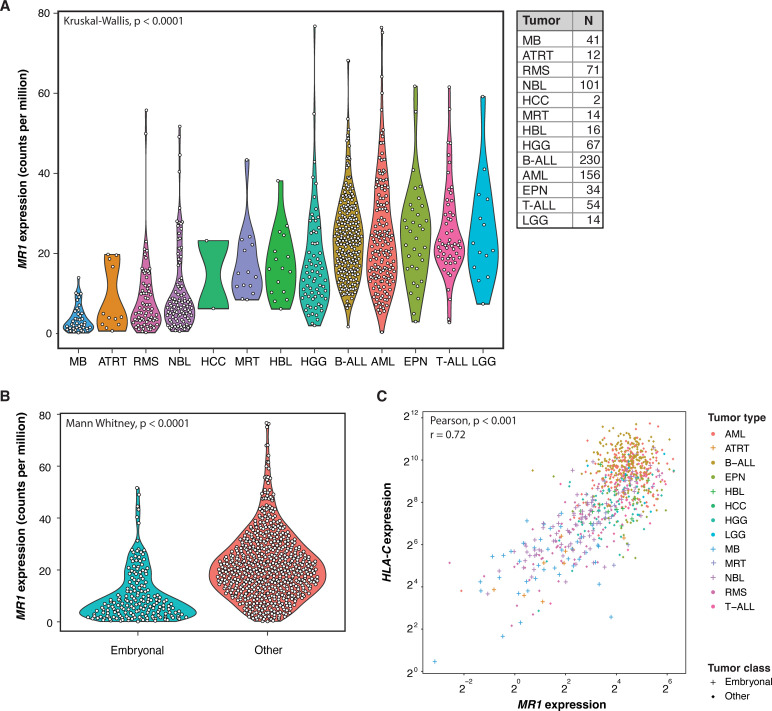
Human leukocyte antigen (HLA) restriction of conventional T-cell targeting introduces complexity in generating T-cell therapy strategies for patients with cancer with diverse HLA-backgrounds. A subpopulation of atypical, major histocompatibility complex-I related protein 1 (MR1)-restricted T-cells, distinctive from mucosal-associated invariant T-cells (MAITs), was recently identified recognizing currently unidentified MR1-presented cancer-specific metabolites. It is hypothesized that the MC.7.G5 MR1T-clone has potential as a pan-cancer, pan-population T-cell immunotherapy approach. These cells are irresponsive to healthy tissue while conferring T-cell receptor(TCR) dependent, HLA-independent cytotoxicity to a wide range of adult cancers. Studies so far are limited to adult malignancies. Here, we investigated the potential of MR1-targeting cellular therapy strategies in pediatric cancer. Bulk RNA sequencing data of primary pediatric tumors were analyzed to assess MR1 expression. In vitro pediatric tumor models were subsequently screened to evaluate their susceptibility to engineered MC.7.G5 TCR-expressing T-cells. Targeting capacity was correlated with qPCR-based MR1 mRNA and protein overexpression. RNA expression of MR1 in primary pediatric tumors varied widely within and between tumor entities. Notably, embryonal tumors exhibited significantly lower MR1 expression than other pediatric tumors. In line with this, most screened embryonal tumors displayed resistance to MR1T-targeting in vitro MR1T susceptibility was observed particularly in pediatric leukemia and diffuse midline glioma models. This study demonstrates potential of MC.7.G5 MR1T-cell immunotherapy in pediatric leukemias and diffuse midline glioma, while activity against embryonal tumors was limited. The dismal prognosis associated with relapsed/refractory leukemias and high-grade brain tumors highlights the promise to improve survival rates of children with these cancers.
Keywords: cell engineering; immunotherapy; pediatrics.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ZS and JK are inventors on different patents for γδ TCR sequences, recognition mechanisms and isolation strategies. JK is scientific cofounder and shareholder of Gadeta (www.gadeta.nl). The remaining authors declare no competing interests.
Figures

References
-
- Riegert P, Wanner V, Bahram S. Genomics, isoforms, expression, and phylogeny of the MHC class I-related MR1 gene. J Immunol 1998;161:4066–77. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials