

Inhibition of IL-25/IL-17RA improves immune-related adverse events of checkpoint inhibitors and reveals antitumor activity
- PMID: 38519059
- PMCID: PMC10961528
- DOI: 10.1136/jitc-2023-008482
Inhibition of IL-25/IL-17RA improves immune-related adverse events of checkpoint inhibitors and reveals antitumor activity
Abstract
Background: Immune checkpoint inhibitors (ICIs) have improved outcomes and extended patient survival in several tumor types. However, ICIs often induce immune-related adverse events (irAEs) that warrant therapy cessation, thereby limiting the overall effectiveness of this class of therapeutic agents. Currently, available therapies used to treat irAEs might also blunt the antitumor activity of the ICI themselves. Therefore, there is an urgent need to identify treatments that have the potential to be administered alongside ICI to optimize their use.
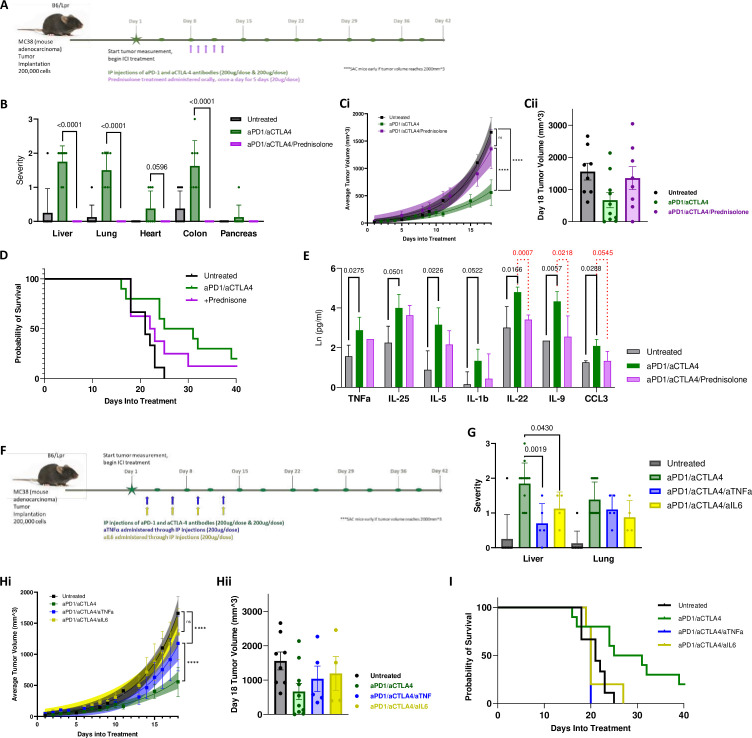
Methods: Using a translationally relevant murine model of anti-PD-1 and anti-CTLA-4 antibodies-induced irAEs, we compared the safety and efficacy of prednisolone, anti-IL-6, anti-TNFɑ, anti-IL-25 (IL-17E), and anti-IL-17RA (the receptor for IL-25) administration to prevent irAEs and to reduce tumor size.
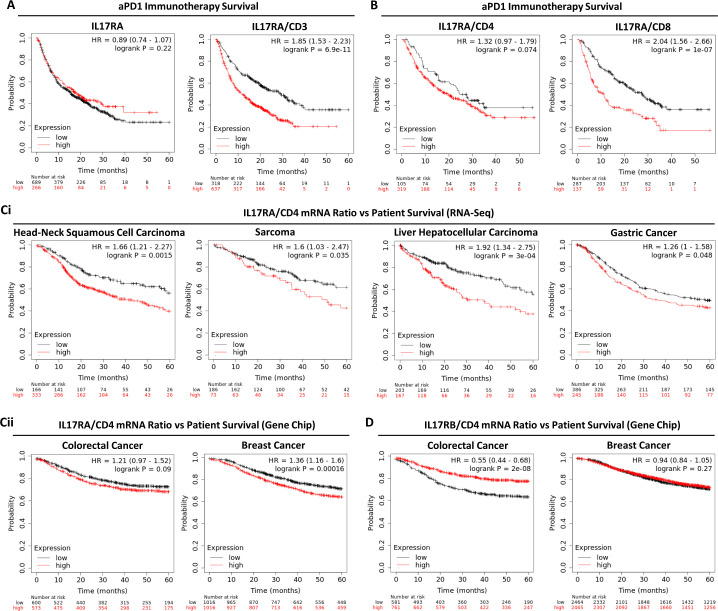
Results: While all interventions were adequate to inhibit the onset of irAEs pneumonitis and hepatitis, treatment with anti-IL-25 or anti-IL-17RA antibodies also exerted additional antitumor activity. Mechanistically, IL-25/IL-17RA blockade reduced the number of organ-infiltrating lymphocytes.
Conclusion: These findings suggest that IL-25/IL-17RA may serve as an additional target when treating ICI-responsive tumors, allowing for better tumor control while suppressing immune-related toxicities.
Keywords: Immune Checkpoint Inhibitors; Immunotherapy; Ipilimumab; Nivolumab; T-Lymphocytes.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AM and XH invented a patent from this study but held no financial interests.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical