

Machine learning-enabled maternal risk assessment for women with pre-eclampsia (the PIERS-ML model): a modelling study
- PMID: 38519152
- PMCID: PMC10983826
- DOI: 10.1016/S2589-7500(23)00267-4
Machine learning-enabled maternal risk assessment for women with pre-eclampsia (the PIERS-ML model): a modelling study
Abstract
Background: Affecting 2-4% of pregnancies, pre-eclampsia is a leading cause of maternal death and morbidity worldwide. Using routinely available data, we aimed to develop and validate a novel machine learning-based and clinical setting-responsive time-of-disease model to rule out and rule in adverse maternal outcomes in women presenting with pre-eclampsia.
Methods: We used health system, demographic, and clinical data from the day of first assessment with pre-eclampsia to predict a Delphi-derived composite outcome of maternal mortality or severe morbidity within 2 days. Machine learning methods, multiple imputation, and ten-fold cross-validation were used to fit models on a development dataset (75% of combined published data of 8843 patients from 11 low-income, middle-income, and high-income countries). Validation was undertaken on the unseen 25%, and an additional external validation was performed in 2901 inpatient women admitted with pre-eclampsia to two hospitals in south-east England. Predictive risk accuracy was determined by area-under-the-receiver-operator characteristic (AUROC), and risk categories were data-driven and defined by negative (-LR) and positive (+LR) likelihood ratios.
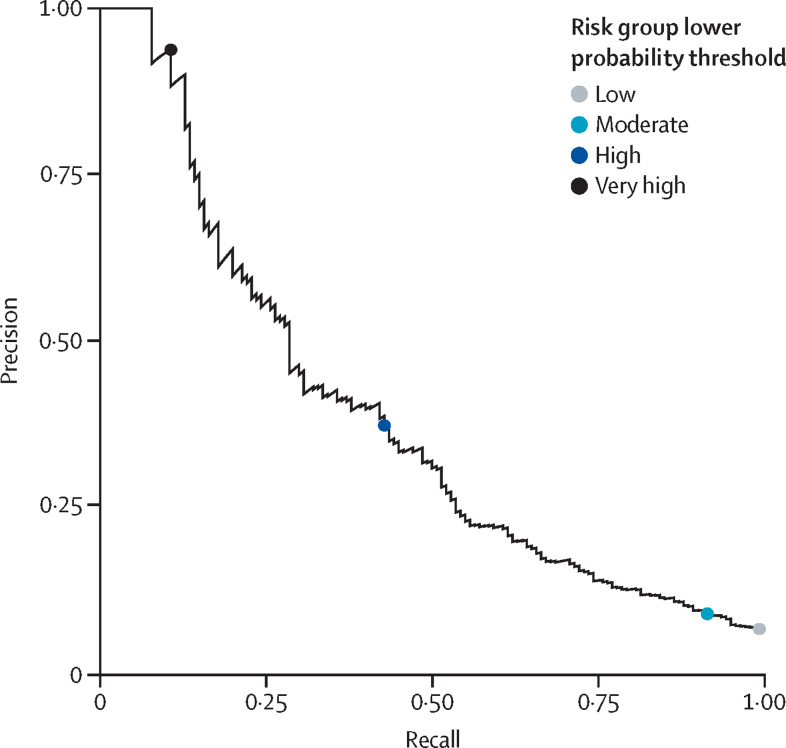
Findings: Of 8843 participants, 590 (6·7%) developed the composite adverse maternal outcome within 2 days, 813 (9·2%) within 7 days, and 1083 (12·2%) at any time. An 18-variable random forest-based prediction model, PIERS-ML, was accurate (AUROC 0·80 [95% CI 0·76-0·84] vs the currently used logistic regression model, fullPIERS: AUROC 0·68 [0·63-0·74]) and categorised women into very low risk (-LR <0·1; eight [0·7%] of 1103 women), low risk (-LR 0·1 to 0·2; 321 [29·1%] women), moderate risk (-LR >0·2 and +LR <5·0; 676 [61·3%] women), high risk (+LR 5·0 to 10·0, 87 [7·9%] women), and very high risk (+LR >10·0; 11 [1·0%] women). Adverse maternal event rates were 0% for very low risk, 2% for low risk, 5% for moderate risk, 26% for high risk, and 91% for very high risk within 48 h. The 2901 women in the external validation dataset were accurately classified as being at very low risk (0% with outcomes), low risk (1%), moderate risk (4%), high risk (33%), or very high risk (67%).
Interpretation: The PIERS-ML model improves identification of women with pre-eclampsia who are at lowest and greatest risk of severe adverse maternal outcomes within 2 days of assessment, and can support provision of accurate guidance to women, their families, and their maternity care providers.
Funding: University of Strathclyde Diversity in Data Linkage Centre for Doctoral Training, the Fetal Medicine Foundation, The Canadian Institutes of Health Research, and the Bill & Melinda Gates Foundation.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TM-C, KK, PM, SJEB, LAM, and PvD acknowledge that the intellectual property related to the PIERS-ML model has been registered, and that the inventors have no financial benefit from the use of the model based on the transfer. TM-C was funded by the University of Strathclyde, through the STRADDLE (University of Strathclyde Diversity in Data Linkage) Centre for Doctoral Training. All other authors declare no competing interests.
Figures




References
-
- Magee LA, Brown MA, Hall DR, et al. The 2021 International Society for the Study of Hypertension in Pregnancy classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2022;27:148–169. - PubMed
-
- Magee LA, Nicolaides KH, von Dadelszen P. Preeclampsia. N Engl J Med. 2022;386:1817–1832. - PubMed
-
- Payne BA, Hutcheon JA, Ansermino JM, et al. A risk prediction model for the assessment and triage of women with hypertensive disorders of pregnancy in low-resourced settings: the miniPIERS (Pre-eclampsia Integrated Estimate of RiSk) multi-country prospective cohort study. PLoS Med. 2014;11 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
