

An international phase II trial and immune profiling of SBRT and atezolizumab in advanced pretreated colorectal cancer
- PMID: 38519913
- PMCID: PMC10960440
- DOI: 10.1186/s12943-024-01970-8
An international phase II trial and immune profiling of SBRT and atezolizumab in advanced pretreated colorectal cancer
Abstract
Background: Immuno-radiotherapy may improve outcomes for patients with advanced solid tumors, although optimized combination modalities remain unclear. Here, we report the colorectal (CRC) cohort analysis from the SABR-PDL1 trial that evaluated the PD-L1 inhibitor atezolizumab in combination with stereotactic body radiation therapy (SBRT) in advanced cancer patients.
Methods: Eligible patients received atezolizumab 1200 mg every 3 weeks until progression or unmanageable toxicity, together with ablative SBRT delivered concurrently with the 2nd cycle (recommended dose of 45 Gy in 3 fractions, adapted upon normal tissue tolerance constraint). SBRT was delivered to at least one tumor site, with at least one additional measurable lesion being kept from the radiation field. The primary efficacy endpoint was one-year progression-free survival (PFS) rate from the start of atezolizumab. Sequential tumor biopsies were collected for deep multi-feature immune profiling.
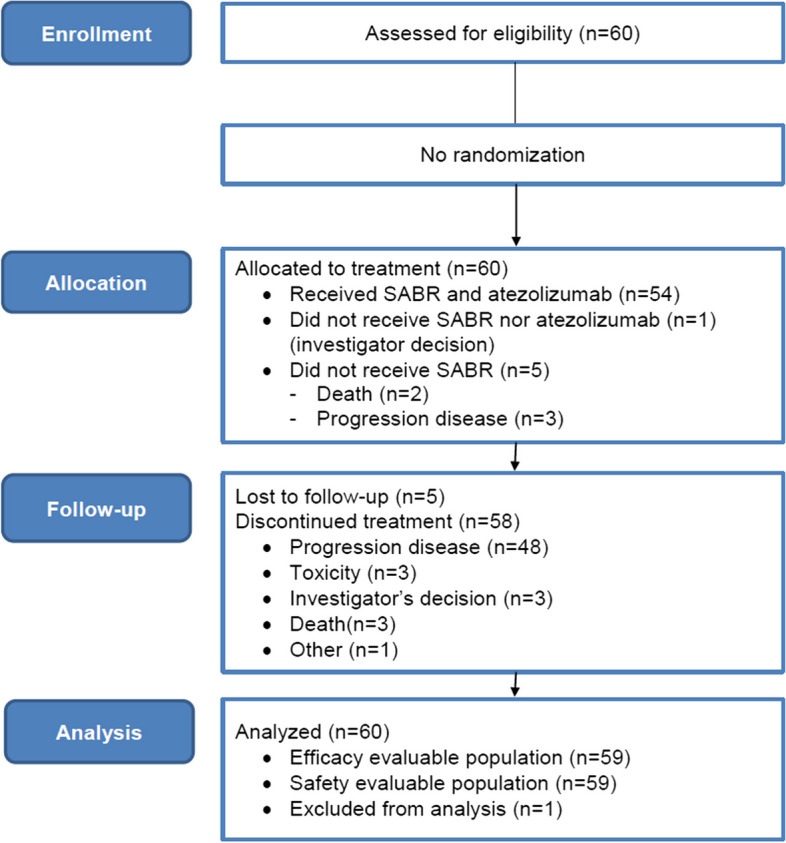
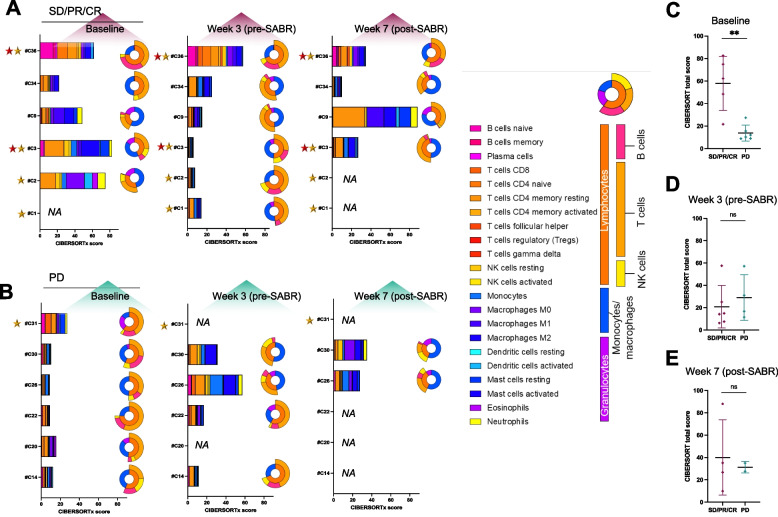
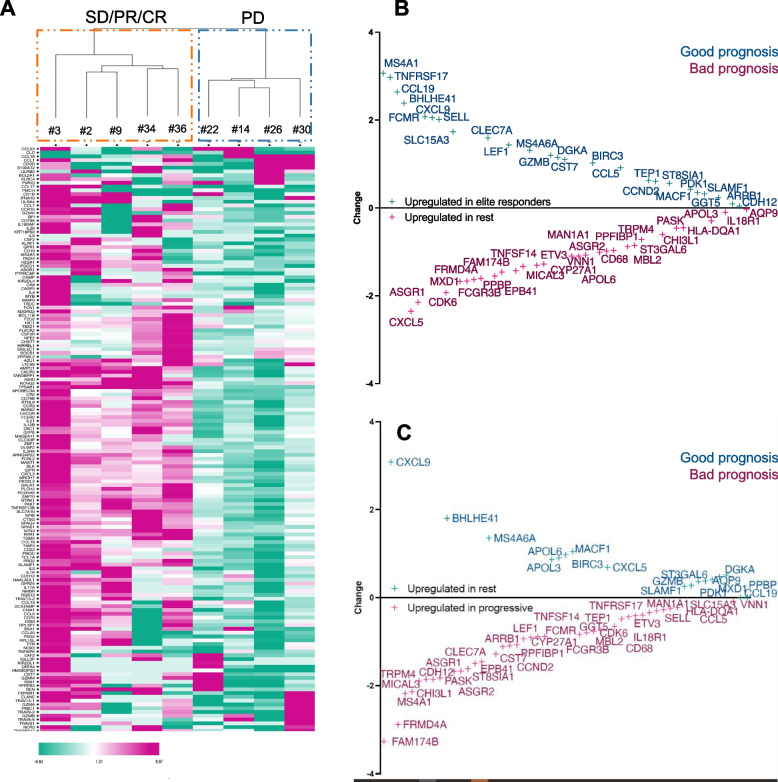
Results: Sixty pretreated (median of 2 prior lines) advanced CRC patients (38 men [63%]; median age, 59 years [range, 20-81 years]; 77% with liver metastases) were enrolled in five centers (France: n = 4, Spain: n = 1) from 11/2016 to 04/2019. All but one (98%) received atezolizumab and 54/60 (90%) received SBRT. The most frequently irradiated site was lung (n = 30/54; 56.3%). Treatment-related G3 (no G4-5) toxicity was observed in 3 (5%) patients. Median OS and PFS were respectively 8.4 [95%CI:5.9-11.6] and 1.4 months [95%CI:1.2-2.6], including five (9%) patients with PFS > 1 year (median time to progression: 19.2 months, including 2/5 MMR-proficient). Best overall responses consisted of stable disease (n = 38; 64%), partial (n = 3; 5%) and complete response (n = 1; 2%). Immune-centric multiplex IHC and RNAseq showed that SBRT redirected immune cells towards tumor lesions, even in the case of radio-induced lymphopenia. Baseline tumor PD-L1 and IRF1 nuclear expression (both in CD3 + T cells and in CD68 + cells) were higher in responding patients. Upregulation of genes that encode for proteins known to increase T and B cell trafficking to tumors (CCL19, CXCL9), migration (MACF1) and tumor cell killing (GZMB) correlated with responses.
Conclusions: This study provides new data on the feasibility, efficacy, and immune context of tumors that may help identifying advanced CRC patients most likely to respond to immuno-radiotherapy.
Trial registration: EudraCT N°: 2015-005464-42; Clinicaltrial.gov number: NCT02992912.
© 2024. The Author(s).
Conflict of interest statement
E.D. reports grants and personal fees from Roche-Genentech, grants and personal fees from AstraZeneca, grants and personal fees from Merck Serono, grants and personal fees from Boehringer, grants and personal fees from BMS, and grants and personal fees from MSD.
N.M. reports grants and personal fees from Merck Serono, grants and personal fees from Bayer, and grants and personal fees from MSD.
A.L. reports grants for academic research from PharMamar, Beigene, Roche, AstraZeneca and Amgen.
L.V. reports personal fees from Adaptherapy, is CEO of RESOLVED, has received non-personal fees from Pierre-Fabre and Servier, and a grant from Bristol-Myers Squibb, all outside the submitted work. Research Grants from Astrazeneca, BMS, Boehringer Ingelheim, Celsius, EIT Philips, GSK, INCA, IDERA, Janssen, Lombard, Merck, MedImmune, Pierre Fabre, Roche, Sanofi, Servier. Non-financial support (drug supplied) from Astrazeneca, BMS, Boringher Ingelheim, GSK, Idera, Medimmune, Merck, NH Theraguix, Roche.
M.R. reports receiving research funding from Roche and Highlight Therapeutics. She also has received speaker’s bureau honoraria from BMS and ROCHE.
RS received support from Fondation Bettencourt-Schueller (CCA Inserm-Bettencourt 2020).
C. Quevrin was funded by Ligue Contre le Cancer (Ref IP/SC #17563).
Figures


References
-
- Robert C, Ribas A, Schachter J, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019;20:1239. doi: 10.1016/S1470-2045(19)30388-2. - DOI - PubMed
-
- Le DT, Kim TW, Van Cutsem E, Geva R, Jäger D, Hara H, et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J Clin Oncol. 2020;1(38):11–19. doi: 10.1200/JCO.19.02107. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
