

Sex-specific associations between sodium and potassium intake and overall and cause-specific mortality: a large prospective U.S. cohort study, systematic review, and updated meta-analysis of cohort studies
- PMID: 38519925
- PMCID: PMC10960470
- DOI: 10.1186/s12916-024-03350-x
Sex-specific associations between sodium and potassium intake and overall and cause-specific mortality: a large prospective U.S. cohort study, systematic review, and updated meta-analysis of cohort studies
Abstract
Background: The impact of sodium intake on cardiovascular disease (CVD) health and mortality has been studied for decades, including the well-established association with blood pressure. However, non-linear patterns, dose-response associations, and sex differences in the relationship between sodium and potassium intakes and overall and cause-specific mortality remain to be elucidated and a comprehensive examination is lacking. Our study objective was to determine whether intake of sodium and potassium and the sodium-potassium ratio are associated with overall and cause-specific mortality in men and women.
Methods: We conducted a prospective analysis of 237,036 men and 179,068 women in the National Institutes of Health-AARP Diet and Health Study. Multivariable-adjusted Cox proportional hazard regression models were utilized to calculate hazard ratios. A systematic review and meta-analysis of cohort studies was also conducted.
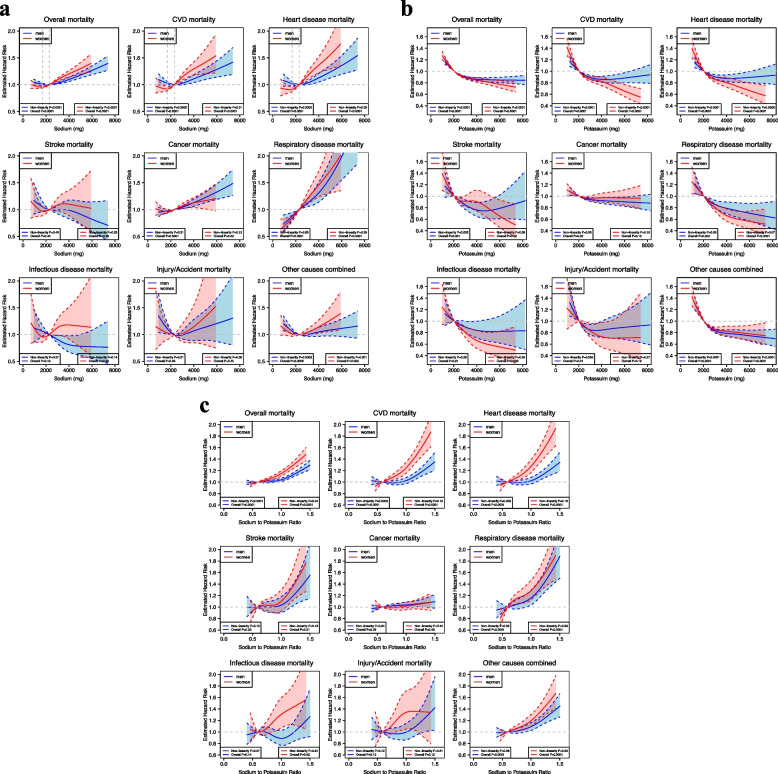
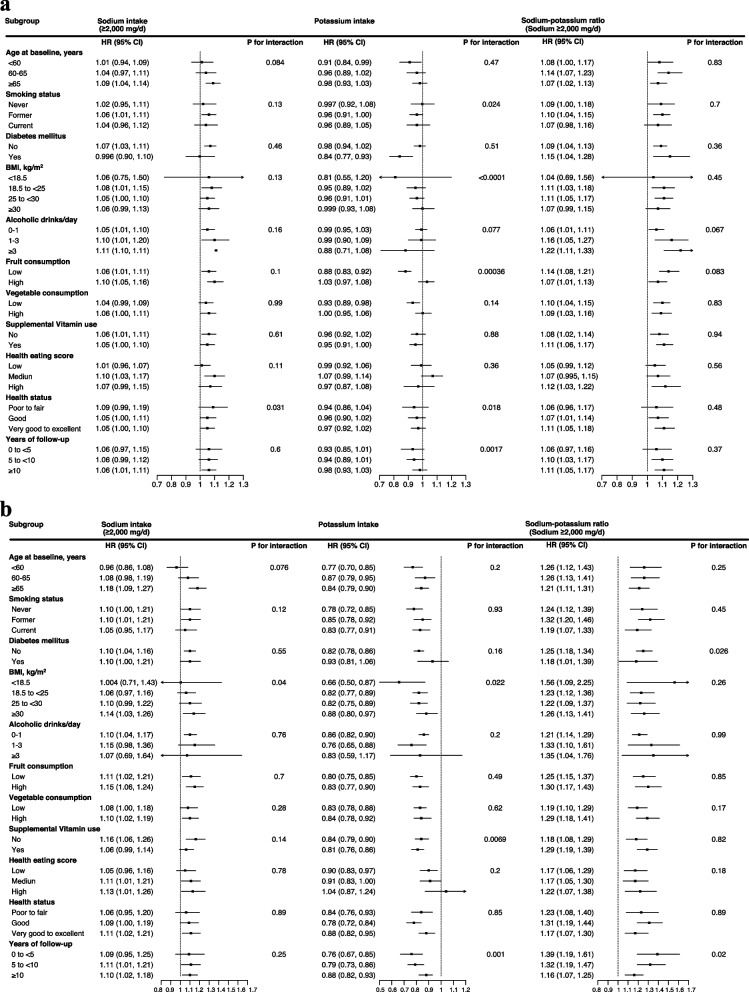
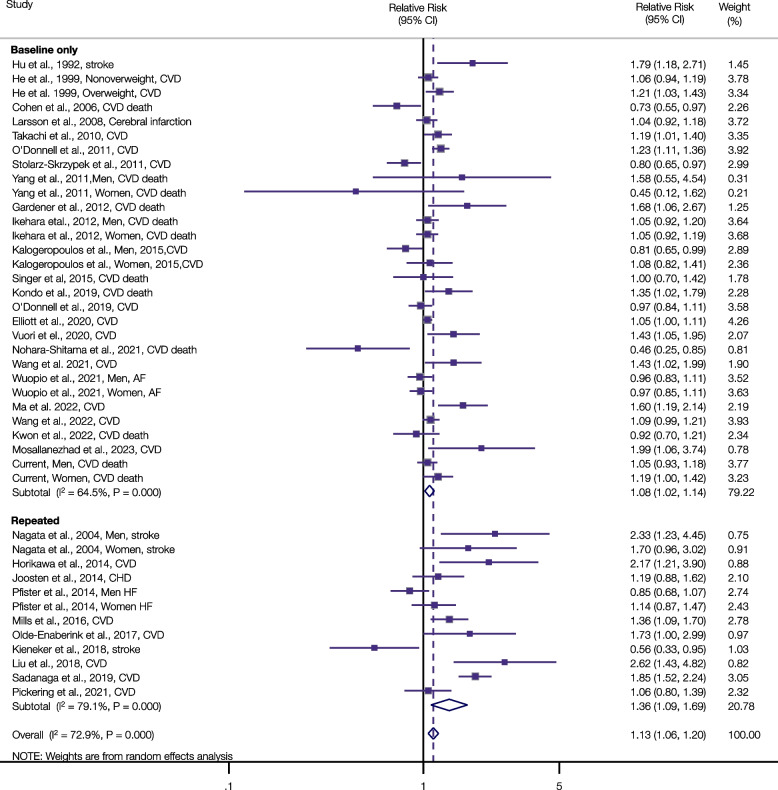
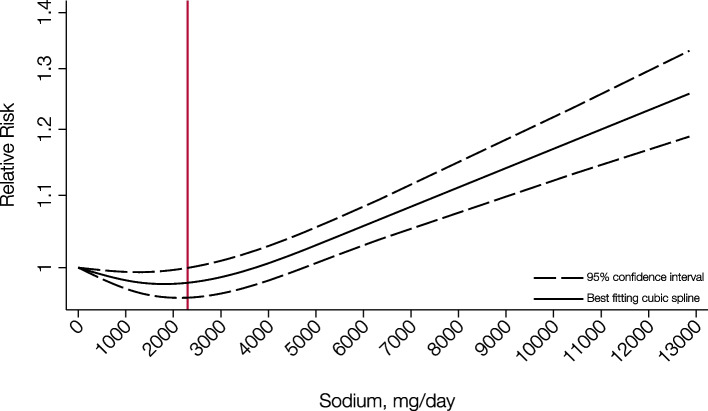
Results: During 6,009,748 person-years of follow-up, there were 77,614 deaths, 49,297 among men and 28,317 among women. Adjusting for other risk factors, we found a significant positive association between higher sodium intake (≥ 2,000 mg/d) and increased overall and CVD mortality (overall mortality, fifth versus lowest quintile, men and women HRs = 1.06 and 1.10, Pnonlinearity < 0.0001; CVD mortality, fifth versus lowest quintile, HRs = 1.07 and 1.21, Pnonlinearity = 0.0002 and 0.01). Higher potassium intake and a lower sodium-potassium ratio were associated with a reduced mortality, with women showing stronger associations (overall mortality, fifth versus lowest quintile, HRs for potassium = 0.96 and 0.82, and HRs for the sodium-potassium ratio = 1.09 and 1.23, for men and women, respectively; Pnonlinearity < 0.05 and both P for interaction ≤ 0.0006). The overall mortality associations with intake of sodium, potassium and the sodium-potassium ratio were generally similar across population risk factor subgroups with the exception that the inverse potassium-mortality association was stronger in men with lower body mass index or fruit consumption (Pinteraction < 0.0004). The updated meta-analysis of cohort studies based on 42 risk estimates, 2,085,904 participants, and 80,085 CVD events yielded very similar results (highest versus lowest sodium categories, pooled relative risk for CVD events = 1.13, 95% CI: 1.06-1.20; Pnonlinearity < 0.001).
Conclusions: Our study demonstrates significant positive associations between daily sodium intake (within the range of sodium intake between 2,000 and 7,500 mg/d), the sodium-potassium ratio, and risk of CVD and overall mortality, with women having stronger sodium-potassium ratio-mortality associations than men, and with the meta-analysis providing compelling support for the CVD associations. These data may suggest decreasing sodium intake and increasing potassium intake as means to improve health and longevity, and our data pointing to a sex difference in the potassium-mortality and sodium-potassium ratio-mortality relationships provide additional evidence relevant to current dietary guidelines for the general adult population.
Systematic review registration: PROSPERO Identifier: CRD42022331618.
Keywords: Cause-specific mortality; Multivariate analysis; Overall mortality; Sex-specific; Sodium and potassium intake; Systematic review and meta-analysis.
© 2024. The Author(s).
Conflict of interest statement
All author declare that they have no potential conflicts of interest.
Figures
References
-
- Jackson SL, Cogswell ME, Zhao L, Terry AL, Wang CY, Wright J, Coleman King SM, Bowman B, Chen TC, Merritt R, et al. Association between urinary sodium and potassium excretion and blood pressure among adults in the United States: National health and nutrition examination survey, 2014. Circulation. 2018;137(3):237–246. doi: 10.1161/CIRCULATIONAHA.117.029193. - DOI - PMC - PubMed
-
- Cook NR, Obarzanek E, Cutler JA, Buring JE, Rexrode KM, Kumanyika SK, Appel LJ, Whelton PK, Trials of Hypertension Prevention Collaborative Research G Joint effects of sodium and potassium intake on subsequent cardiovascular disease: the trials of hypertension prevention follow-up study. Arch Intern Med. 2009;169(1):32–40. doi: 10.1001/archinternmed.2008.523. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
