

Transurethral surgical treatment for benign prostatic hyperplasia with detrusor underactivity: a systematic review and meta-analysis
- PMID: 38520009
- PMCID: PMC10958878
- DOI: 10.1186/s13643-024-02514-3
Transurethral surgical treatment for benign prostatic hyperplasia with detrusor underactivity: a systematic review and meta-analysis
Abstract
Background: The efficacy of surgical treatment for benign prostatic hyperplasia (BPH) patients with detrusor underactivity (DU) remains controversial.
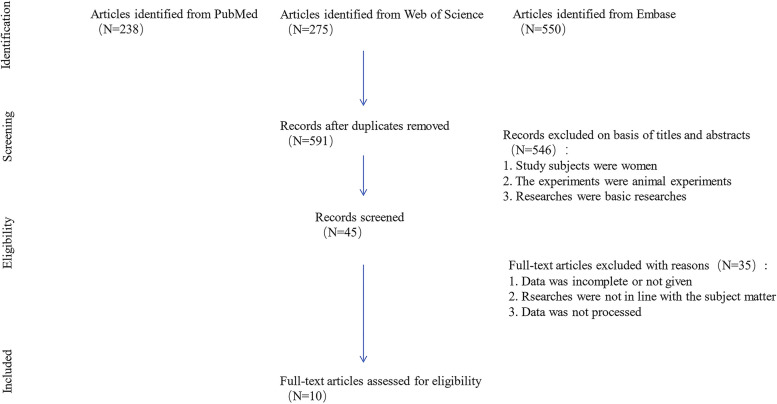
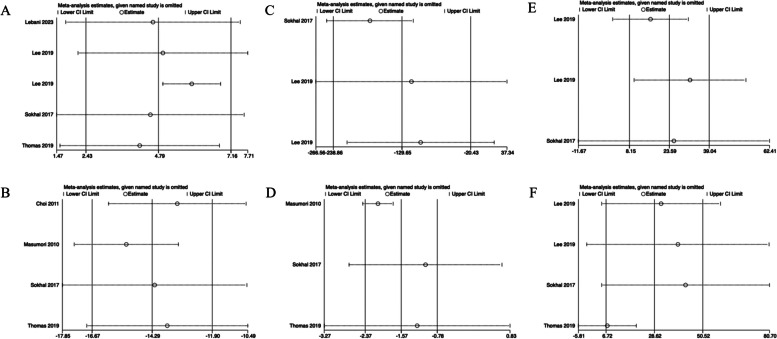
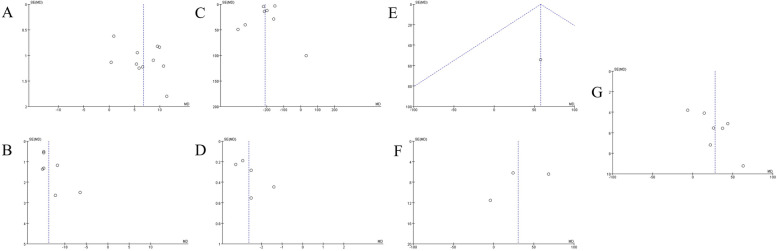
Methods: To summarize relevant evidence, three databases (PubMed, Embase, and Web of Science) were searched from database inception to May 1, 2023. Transurethral surgical treatment modalities include transurethral prostatectomy (TURP), photoselective vaporization of the prostate (PVP), and transurethral incision of the prostate (TUIP). The efficacy of the transurethral surgical treatment was assessed according to maximal flow rate on uroflowmetry (Qmax), International Prostate Symptom Score (IPSS), postvoid residual (PVR), quality of life (QoL), voided volume, bladder contractility index (BCI) and maximal detrusor pressure at maximal flow rate (PdetQmax). Pooled mean differences (MDs) were used as summary statistics for comparison. The quality of enrolled studies was evaluated by using the Newcastle-Ottawa Scale. Sensitivity analysis and funnel plots were applied to assess possible biases.
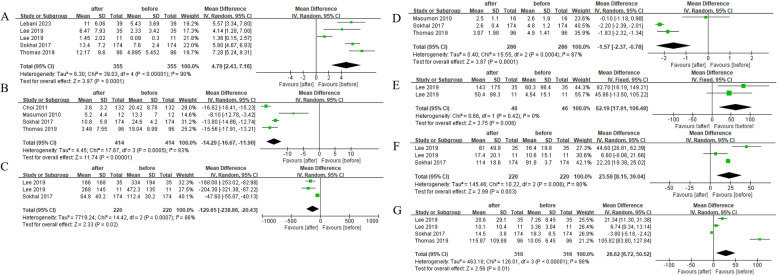
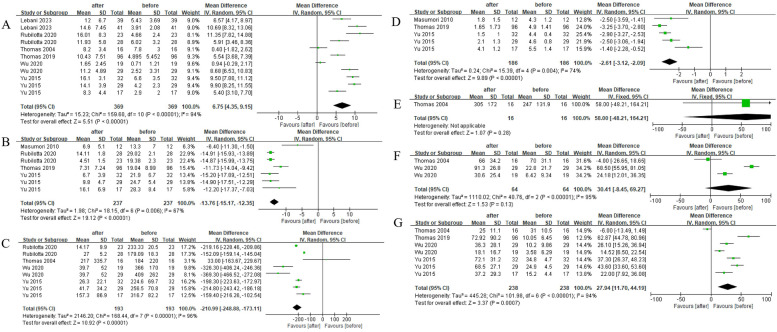
Results: In this study, 10 studies with a total of 1142 patients enrolled. In BPH patients with DU, within half a year, significant improvements in Qmax (pooled MD, 4.79; 95% CI, 2.43-7.16; P < 0.05), IPSS(pooled MD, - 14.29; 95%CI, - 16.67-11.90; P < 0.05), QoL (pooled MD, - 1.57; 95% CI, - 2.37-0.78; P < 0.05), voided volume (pooled MD, 62.19; 95% CI, 17.91-106.48; P < 0.05), BCI (pooled MD, 23.59; 95% CI, 8.15-39.04; P < 0.05), and PdetQmax (pooled MD, 28.62; 95% CI, 6.72-50.52; P < 0.05) were observed after surgery. In addition, after more than 1 year, significant improvements were observed in Qmax (pooled MD, 6.75; 95%CI, 4.35-9.15; P < 0.05), IPSS(pooled MD, - 13.76; 95%CI, - 15.17-12.35; P < 0.05), PVR (pooled MD, - 179.78; 95%CI, - 185.12-174.44; P < 0.05), QoL (pooled MD, - 2.61; 95%CI, - 3.12-2.09; P < 0.05), and PdetQmax (pooled MD, 27.94; 95%CI, 11.70-44.19; P < 0.05). Compared with DU patients who did not receive surgery, DU patients who received surgery showed better improvement in PVR (pooled MD, 137.00; 95%CI, 6.90-267.10; P < 0.05) and PdetQmax (pooled MD, - 8.00; 95%CI, - 14.68-1.32; P < 0.05).
Conclusions: Our meta-analysis results showed that transurethral surgery can improve the symptoms of BPH patients with DU. Surgery also showed advantages over pharmacological treatment for BPH patients with DU.
Systematic review registration: PROSPERO CRD42023415188.
Keywords: Detrusor underactivity; Meta-analysis; Systematic review; Transurethral surgical treatment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Functional and safety outcomes after benign prostatic enlargement surgeries in men with detrusor underactivity compared with normal detrusor contractility: Systematic review and meta-analysis.Neurourol Urodyn. 2024 Jan;43(1):126-143. doi: 10.1002/nau.25336. Epub 2023 Nov 27. Neurourol Urodyn. 2024. PMID: 38010924
-
A systematic review and meta-analysis of efficacy and safety comparing greenlight laser vaporization with transurethral resection of the prostate for benign prostatic hyperplasia with prostate volume less than 80 ml.Lasers Med Sci. 2023 Jun 8;38(1):133. doi: 10.1007/s10103-023-03794-2. Lasers Med Sci. 2023. PMID: 37289405
-
Minimally invasive treatments for lower urinary tract symptoms in men with benign prostatic hyperplasia: a network meta-analysis.Cochrane Database Syst Rev. 2021 Jul 15;7(7):CD013656. doi: 10.1002/14651858.CD013656.pub2. Cochrane Database Syst Rev. 2021. PMID: 34693990 Free PMC article.
-
Photoselective vaporization of the prostate with GreenLight 120-W laser versus transurethral resection of the prostate for benign prostatic hyperplasia: a systematic review with meta-analysis of randomized controlled trials.Lasers Med Sci. 2016 Feb;31(2):235-40. doi: 10.1007/s10103-015-1843-1. Epub 2015 Dec 28. Lasers Med Sci. 2016. PMID: 26712715
-
Prostatic arterial embolization for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia.Cochrane Database Syst Rev. 2022 Mar 29;3(3):CD012867. doi: 10.1002/14651858.CD012867.pub3. Cochrane Database Syst Rev. 2022. PMID: 35349161 Free PMC article.
Cited by
-
The association between lower urinary tract symptoms secondary to benign prostatic hyperplasia and multimorbidity among Chinese middle-aged and elderly males: evidence based on propensity score matching.Transl Androl Urol. 2024 Sep 30;13(9):1932-1945. doi: 10.21037/tau-24-268. Epub 2024 Sep 26. Transl Androl Urol. 2024. PMID: 39434733 Free PMC article.
References
-
- Osman NI, Chapple CR, Abrams P, Dmochowski R, Haab F, Nitti V, et al. Detrusor underactivity and the underactive bladder: a new clinical entity? A review of current terminology, definitions, epidemiology, aetiology, and diagnosis. Eur Urol. 2014;65(2):389–398. doi: 10.1016/j.eururo.2013.10.015. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
