

A highly selective mPGES-1 inhibitor to block abdominal aortic aneurysm progression in the angiotensin mouse model
- PMID: 38521811
- PMCID: PMC10960802
- DOI: 10.1038/s41598-024-57437-9
A highly selective mPGES-1 inhibitor to block abdominal aortic aneurysm progression in the angiotensin mouse model
Abstract
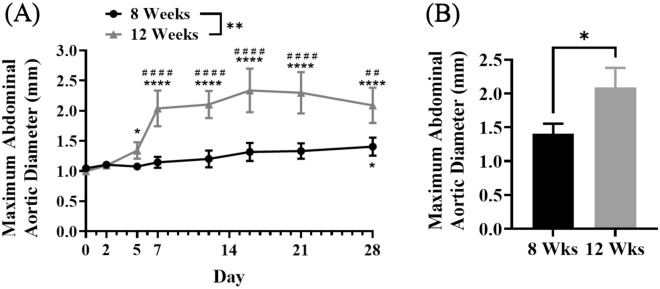
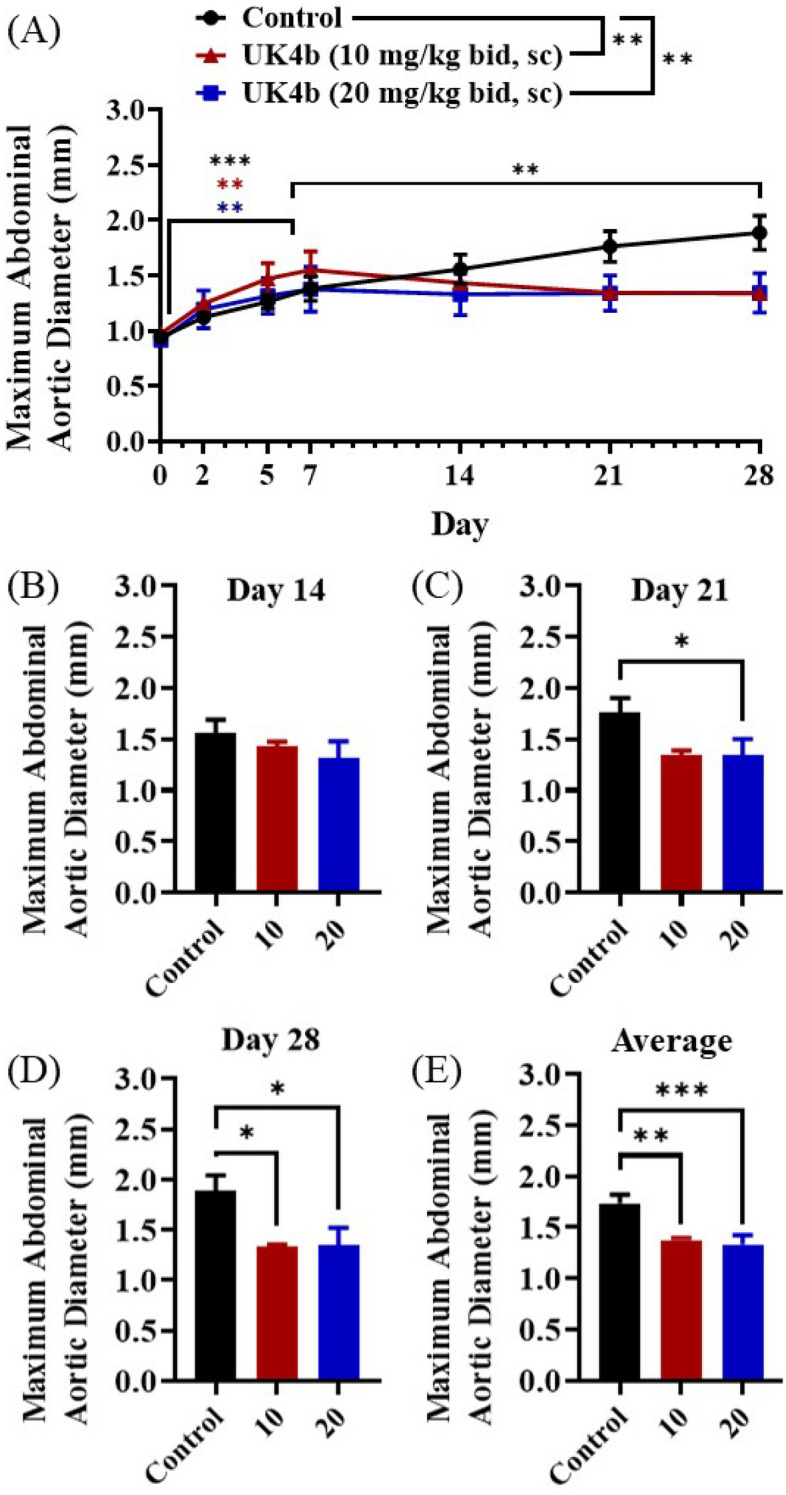
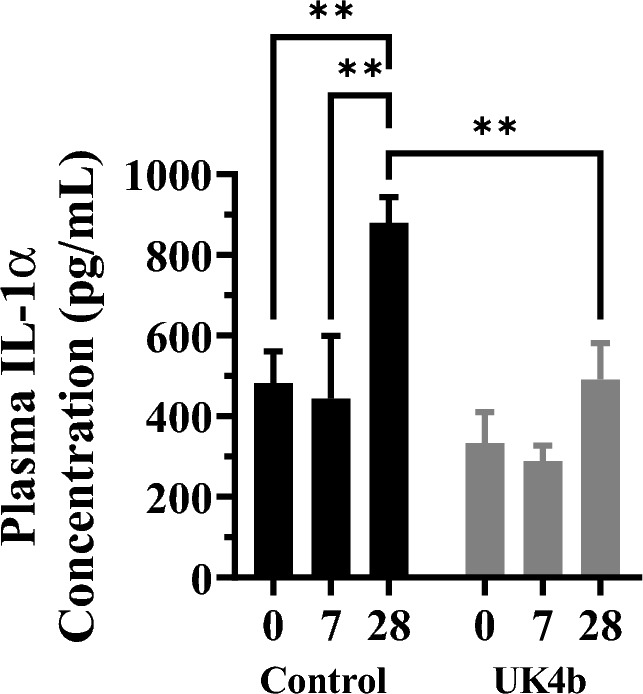
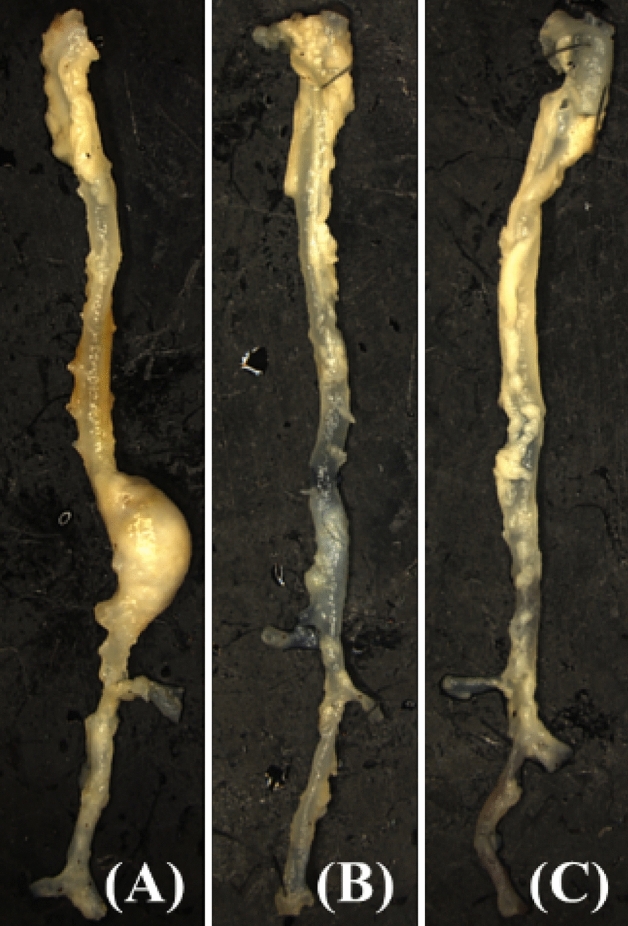
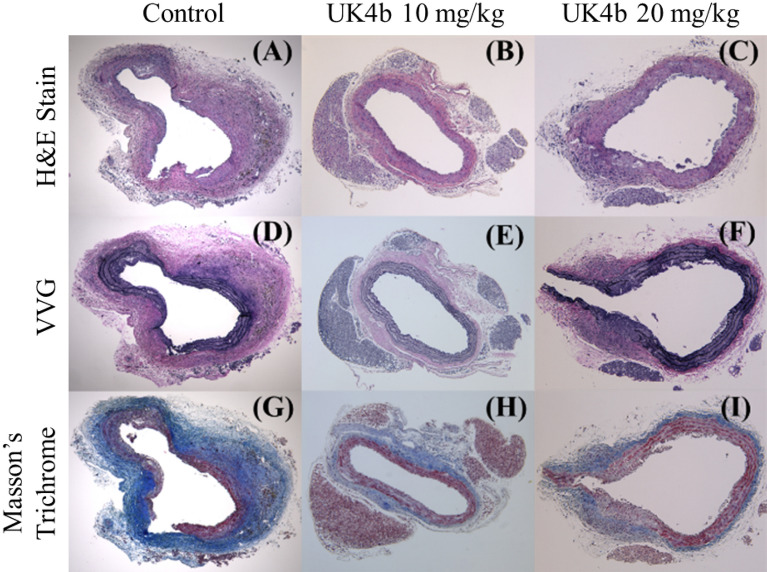
Abdominal aortic aneurysm (AAA) is a deadly, permanent ballooning of the aortic artery. Pharmacological and genetic studies have pointed to multiple proteins, including microsomal prostaglandin E2 synthase-1 (mPGES-1), as potentially promising targets. However, it remains unknown whether administration of an mPGES-1 inhibitor can effectively attenuate AAA progression in animal models. There are still no FDA-approved pharmacological treatments for AAA. Current research stresses the importance of both anti-inflammatory drug targets and rigor of translatability. Notably, mPGES-1 is an inducible enzyme responsible for overproduction of prostaglandin E2 (PGE2)-a well-known principal pro-inflammatory prostanoid. Here we demonstrate for the first time that a highly selective mPGES-1 inhibitor (UK4b) can completely block further growth of AAA in the ApoE-/- angiotensin (Ang)II mouse model. Our findings show promise for the use of a mPGES-1 inhibitor like UK4b as interventional treatment of AAA and its potential translation into the clinical setting.
Keywords: Abdominal aortic aneurysm; Aneurysm; Anti-inflammation; Prostaglandin E2; mPGES-1 inhibitor.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Health service costs and quality of life for early elective surgery or ultrasonographic surveillance for small abdominal aortic aneurysms. UK Small Aneurysm Trial Participants. Lancet1998, 352 (9141), 1656–1660. From NLM. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
