

Meta-analysis and trial sequential analysis of pancreatic stump closure using a hand-sewn or stapler technique in distal pancreatectomy
- PMID: 38522846
- PMCID: PMC11341886
- DOI: 10.14701/ahbps.24-015
Meta-analysis and trial sequential analysis of pancreatic stump closure using a hand-sewn or stapler technique in distal pancreatectomy
Abstract
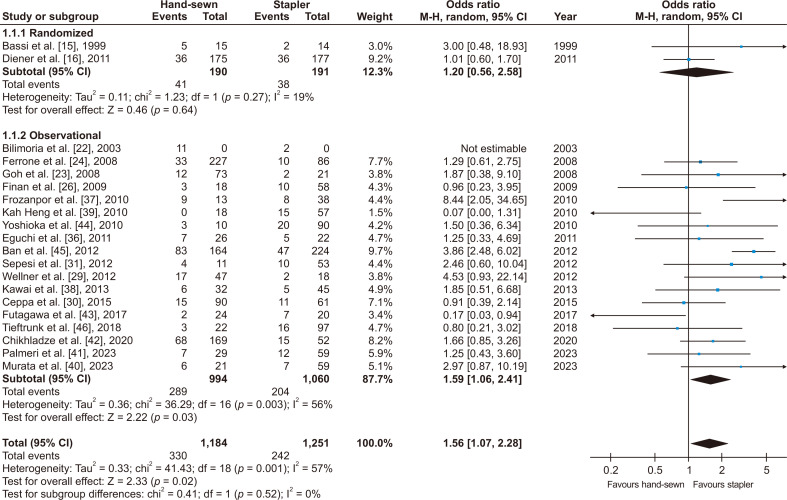
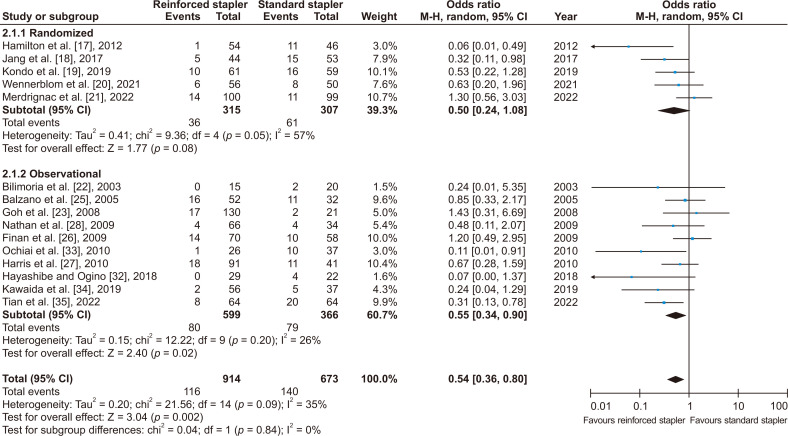
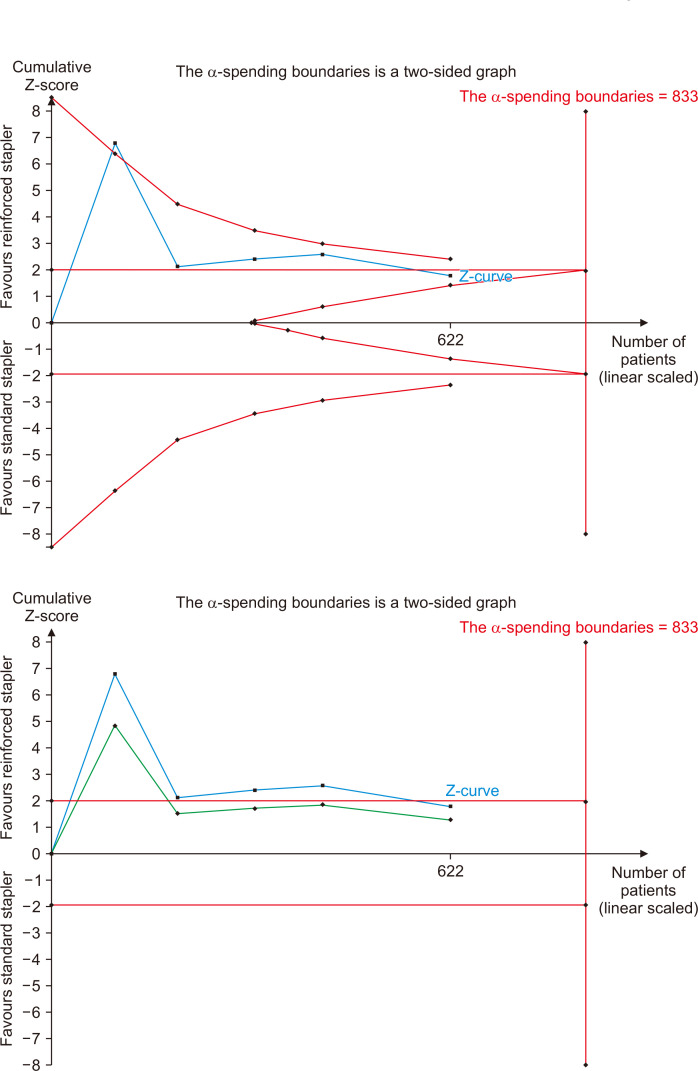
This study aimed to compare outcomes of hand-sewn and stapler closure techniques of pancreatic stump in patients undergoing distal pancreatectomy (DP). Impact of stapler closure reinforcement using mesh on outcomes was also evaluated. Literature search was carried out using multiple data sources to identify studies that compared hand-sewn and stapler closure techniques in management of pancreatic stump following DP. Odds ratio (OR) was determined for clinically relevant postoperative pancreatic fistula (POPF) via random-effects modelling. Subsequently, trial sequential analysis was performed. Thirty-two studies with a total of 4,022 patients undergoing DP with hand-sewn (n = 1,184) or stapler (n = 2,838) closure technique of pancreatic stump were analyzed. Hand-sewn closure significantly increased the risk of clinically relevant POPF compared to stapler closure (OR: 1.56, p = 0.02). When stapler closure was considered, staple line reinforcement significantly reduced formation of such POPF (OR: 0.54, p = 0.002). When only randomized controlled trials were considered, there was no significant difference in clinically relevant POPF between hand-sewn and stapler closure techniques (OR: 1.20, p = 0.64) or between reinforced and standard stapler closure techniques (OR: 0.50, p = 0.08). When observational studies were considered, hand-sewn closure was associated with a significantly higher rate of clinically relevant POPF compared to stapler closure (OR: 1.59, p = 0.03). Moreover, when stapler closure was considered, staple line reinforcement significantly reduced formation of such POPF (OR: 0.55, p = 0.02). Trial sequential analysis detected risk of type 2 error. In conclusion, reinforced stapler closure in DP may reduce risk of clinically relevant POPF compared to hand-sewn closure or stapler closure without reinforcement. Future randomized research is needed to provide stronger evidence.
Keywords: Distal pancreatectomy; Hand-sewn closure; Pancreatic stump; Stapler closure.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures


Similar articles
-
Efficacy of Reinforced Stapler Versus Hand-sewn Closure of the Pancreatic Stump During Pure Laparoscopic Distal Pancreatectomy to Reduce Pancreatic Fistula.Surg Laparosc Endosc Percutan Tech. 2023 Apr 1;33(2):99-107. doi: 10.1097/SLE.0000000000001151. Surg Laparosc Endosc Percutan Tech. 2023. PMID: 36821651
-
Efficacy of pancreaticojejunostomy of the pancreatic stump during distal or central pancreatectomy.Langenbecks Arch Surg. 2024 Apr 30;409(1):145. doi: 10.1007/s00423-024-03335-7. Langenbecks Arch Surg. 2024. PMID: 38687358
-
Efficacy of stapler versus hand-sewn closure after distal pancreatectomy (DISPACT): a randomised, controlled multicentre trial.Lancet. 2011 Apr 30;377(9776):1514-22. doi: 10.1016/S0140-6736(11)60237-7. Lancet. 2011. PMID: 21529927 Clinical Trial.
-
Network meta-analysis comparing techniques and outcomes of stump closure after distal pancreatectomy.Br J Surg. 2019 Nov;106(12):1580-1589. doi: 10.1002/bjs.11291. Epub 2019 Oct 18. Br J Surg. 2019. PMID: 31626341
-
The outcome of bioabsorbable staple line reinforcement versus standard stapler for distal pancreatectomy: A systematic review and meta-analysis.J Minim Access Surg. 2022 Jul-Sep;18(3):338-345. doi: 10.4103/jmas.jmas_47_22. J Minim Access Surg. 2022. PMID: 35708377 Free PMC article. Review.
Cited by
-
Stapler versus scalpel resection followed by handsewn closure of the pancreatic remnant for distal pancreatectomy.Cochrane Database Syst Rev. 2025 Jun 10;6(6):CD008688. doi: 10.1002/14651858.CD008688.pub3. Cochrane Database Syst Rev. 2025. PMID: 40492489 Review.
-
Italian survey about intraperitoneal drain use in distal pancreatectomy.Updates Surg. 2025 Jan;77(1):9-17. doi: 10.1007/s13304-024-01987-0. Epub 2024 Oct 13. Updates Surg. 2025. PMID: 39397215 Free PMC article.
References
-
- Dhanireddy KK, Fishbein TM. In: Surgical pitfalls e-book: prevention and management. Evans SRT, Chahine AA, editors. Saunders; 2008. Distal pancreatectomy; pp. 375–378. - DOI
-
- Hajibandeh S, Ghassemi N, Hajibandeh S, Romman S, Ghassemi A, Laing RW, et al. Meta-analysis of laparoscopic spleen-preserving distal pancreatectomy versus laparoscopic distal pancreatectomy with splenectomy: an insight into confounding by indication. Surgeon. 2023;22:e13–e25. doi: 10.1016/j.surge.2023.08.006. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources