

Natural history of clonal haematopoiesis seen in real-world haematology settings
- PMID: 38522849
- PMCID: PMC11232927
- DOI: 10.1111/bjh.19423
Natural history of clonal haematopoiesis seen in real-world haematology settings
Abstract
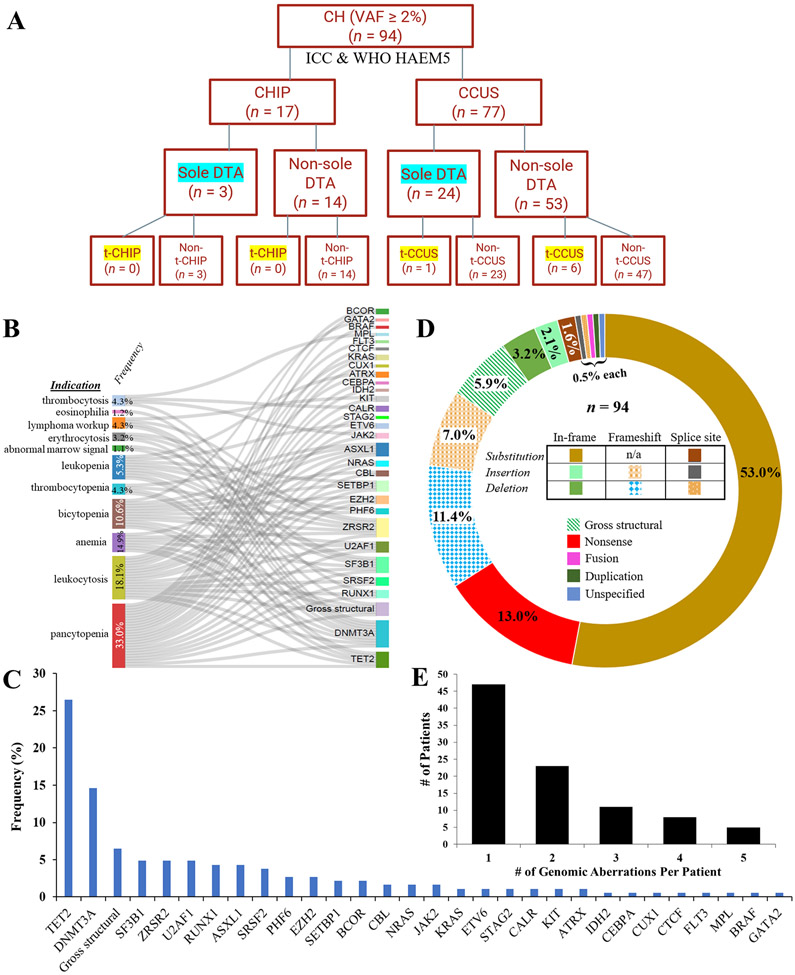
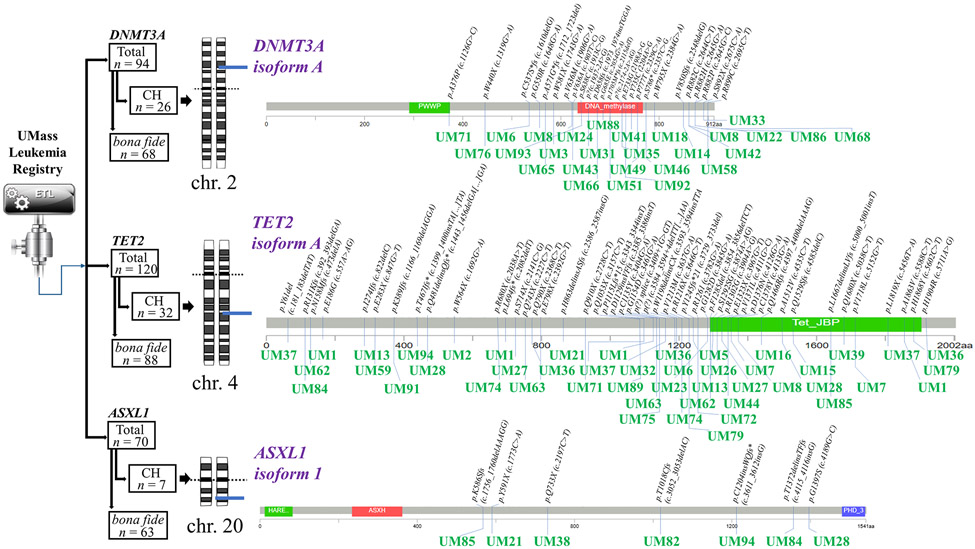
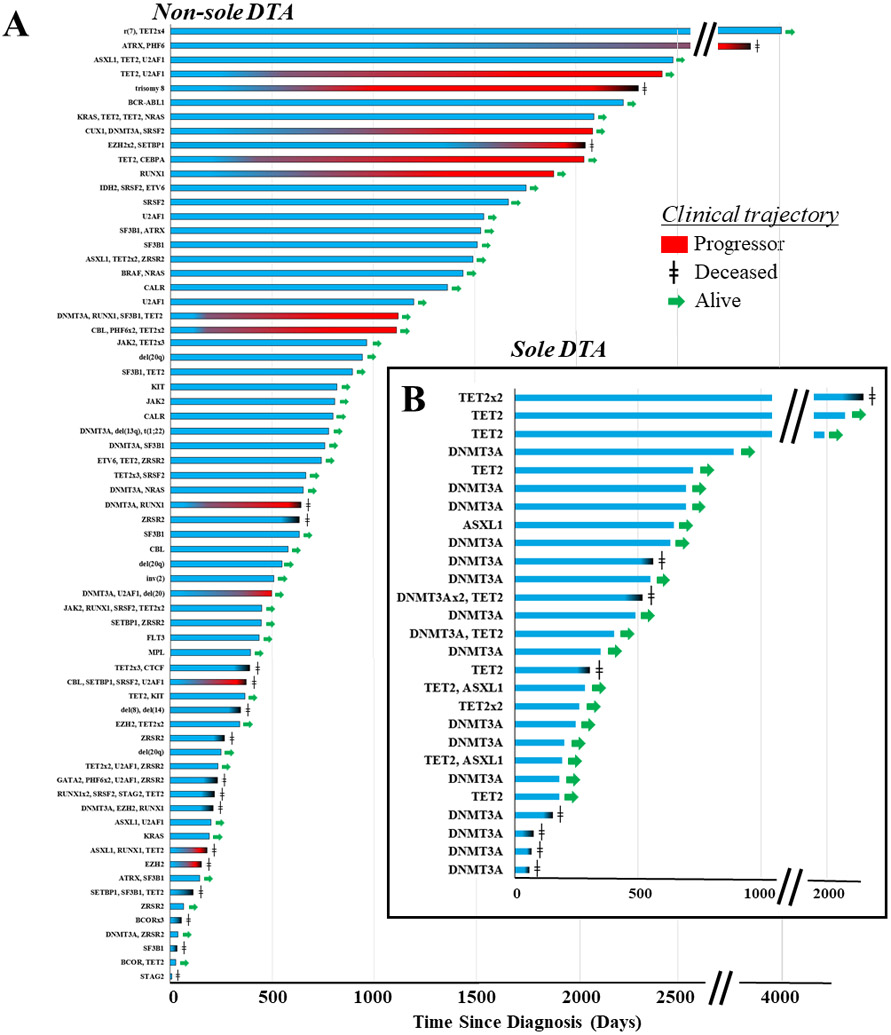
Recursive partitioning of healthy consortia led to the development of the Clonal Hematopoiesis Risk Score (CHRS) for clonal haematopoiesis (CH); however, in the practical setting, most cases of CH are diagnosed after patients present with cytopenias or related symptoms. To address this real-world population, we characterize the clinical trajectories of 94 patients with CH and distinguish CH harbouring canonical DNMT3A/TET2/ASXL1 mutations alone ('sole DTA') versus all other groups ('non-sole DTA'). TET2, rather than DNMT3A, was the most prevalent mutation in the real-world setting. Sole DTA patients did not progress to myeloid neoplasm (MN) in the absence of acquisition of other mutations. Contrastingly, 14 (20.1%) of 67 non-sole DTA patients progressed to MN. CHRS assessment showed a higher frequency of high-risk CH in non-sole DTA (vs. sole DTA) patients and in progressors (vs. non-progressors). RUNX1 mutation conferred the strongest risk for progression to MN (odds ratio [OR] 10.27, 95% CI 2.00-52.69, p = 0.0053). The mean variant allele frequency across all genes was higher in progressors than in non-progressors (36.9% ± 4.62% vs. 24.1% ± 1.67%, p = 0.0064). This analysis in the post-CHRS era underscores the natural history of CH, providing insight into patterns of progression to MN.
Keywords: CHIP; acute myeloid leukaemia; clonal haematopoiesis; epigenetics; myelodysplastic syndrome; myeloid genomics.
© 2024 British Society for Haematology and John Wiley & Sons Ltd.
Figures



References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
