

Secondary Pulmonary Alveolar Proteinosis Development during the Treatment for Anti-aminoacyl-tRNA Synthetase Antibody-positive Interstitial Lung Disease
- PMID: 38522908
- PMCID: PMC11604386
- DOI: 10.2169/internalmedicine.3327-23
Secondary Pulmonary Alveolar Proteinosis Development during the Treatment for Anti-aminoacyl-tRNA Synthetase Antibody-positive Interstitial Lung Disease
Abstract
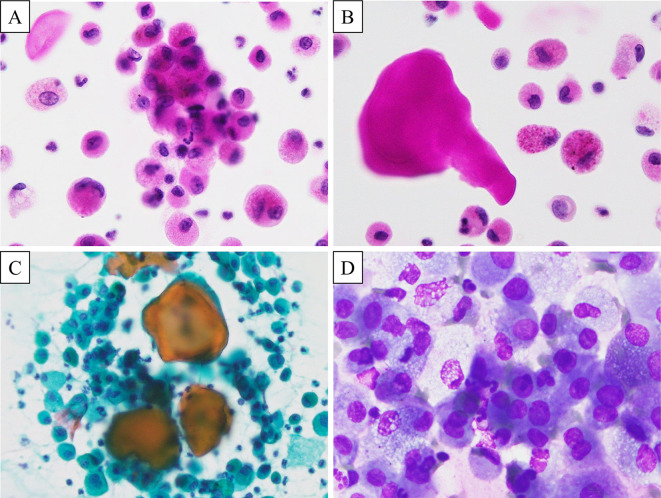
A 70-year-old woman with anti-aminoacyl-tRNA synthetase (ARS) antibody-positive interstitial lung disease (ARS-ILD) received daily medications and regular cyclophosphamide cycles for recurring exacerbations. Approximately four years after immunosuppression initiation, the patient was admitted for progressive dyspnea on exertion. Chest computed tomography (CT) findings were suggestive of acute exacerbation. Despite intensified immunosuppressive treatment, the radiographic findings worsened, and serum Krebs von den Lungen-6 (KL-6) levels increased. A bronchoalveolar lavage fluid (BALF) examination revealed amorphous globules and alveolar macrophages with eosinophilic granules. Owing to negative anti-granulocyte-macrophage colony-stimulating factor antibody tests, a diagnosis of secondary pulmonary alveolar proteinosis (PAP) was established.
Keywords: anti-aminoacyl-tRNA synthetase antibody-positive interstitial lung disease; immunosuppressants; secondary pulmonary alveolar proteinosis; steroid.
Conflict of interest statement
The authors state that they have no Conflict of Interest (COI).
Figures



Similar articles
-
Autoimmune pulmonary alveolar proteinosis exacerbated by steroid therapy due to misdiagnosis as anti-aminoacyl-tRNA synthetase (ARS) antibody positive- interstitial pneumonia: a case report.BMC Pulm Med. 2022 Mar 31;22(1):120. doi: 10.1186/s12890-022-01909-z. BMC Pulm Med. 2022. PMID: 35361191 Free PMC article.
-
Autoimmune pulmonary alveolar proteinosis developed during treatment for systemic sclerosis: a case report.BMC Pulm Med. 2025 Jan 21;25(1):32. doi: 10.1186/s12890-025-03489-0. BMC Pulm Med. 2025. PMID: 39838335 Free PMC article.
-
Autoimmune pulmonary alveolar proteinosis developed during immunosuppressive treatment in polymyositis with interstitial lung disease: a case report.BMC Pulm Med. 2020 Apr 6;20(1):84. doi: 10.1186/s12890-020-1110-5. BMC Pulm Med. 2020. PMID: 32252718 Free PMC article.
-
Bilateral peripheral infiltrates refractory to immunosuppressants were diagnosed as autoimmune pulmonary alveolar proteinosis and improved by inhalation of granulocyte/macrophage-colony stimulating factor.Intern Med. 2012;51(13):1737-42. doi: 10.2169/internalmedicine.51.6093. Epub 2012 Jul 1. Intern Med. 2012. PMID: 22790136 Review.
-
Pulmonary alveolar proteinosis: an overview for internists and hospital physicians.Hosp Pract (1995). 2010 Feb;38(1):43-9. doi: 10.3810/hp.2010.02.277. Hosp Pract (1995). 2010. PMID: 20469623 Review.
Cited by
-
Pulmonary Alveolar Proteinosis During Intensive Immunosuppressive Treatment for Acute Exacerbation of Interstitial Pneumonia: A Case Report and Literature Review.Cureus. 2024 Nov 28;16(11):e74669. doi: 10.7759/cureus.74669. eCollection 2024 Nov. Cureus. 2024. PMID: 39734970 Free PMC article.
References
-
- The Japanese Respiratory Society . In: The JRS Clinical Practice Guideline for Pulmonary Alveolar Proteinosis 2022. 1st ed. Medical Review, Tokyo, 2022: (in Japanese).
-
- Ishii H, Tazawa R, Kaneko C, et al. . Clinical features of secondary pulmonary alveolar proteinosis: pre-mortem cases in Japan. Eur Respir J 37: 465-468, 2011. - PubMed
-
- Seymour JF, Presneill JJ. Pulmonary alveolar proteinosis: progress in the first 44 years. Am J Respir Crit Care Med 166: 215-235, 2002. - PubMed
-
- Imura Y, Yukawa N, Handa T, et al. . Two cases of autoimmune and secondary pulmonary alveolar proteinosis during immunosuppressive therapy in dermatomyositis with interstitial lung disease. Mod Rheumatol 28: 724-729, 2018. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials