

Knee Offloading by Patients During Walking and Running After Meniscectomy
- PMID: 38524891
- PMCID: PMC10958822
- DOI: 10.1177/23259671231214766
Knee Offloading by Patients During Walking and Running After Meniscectomy
Abstract
Background: Changes in knee loading have been reported after meniscectomy. Knee loading has previously been assessed during jogging and treadmill running rather than overground running, which could give altered results.
Purpose/hypothesis: The purpose of this study was to evaluate knee function during overground running and walking after meniscectomy. It was hypothesized that the affected limb would demonstrate higher external knee adduction moment, lower knee flexion moment (KFM), and lower knee rotation moment (KRM) compared with the contralateral limb and with healthy individuals.
Study design: Controlled laboratory study.
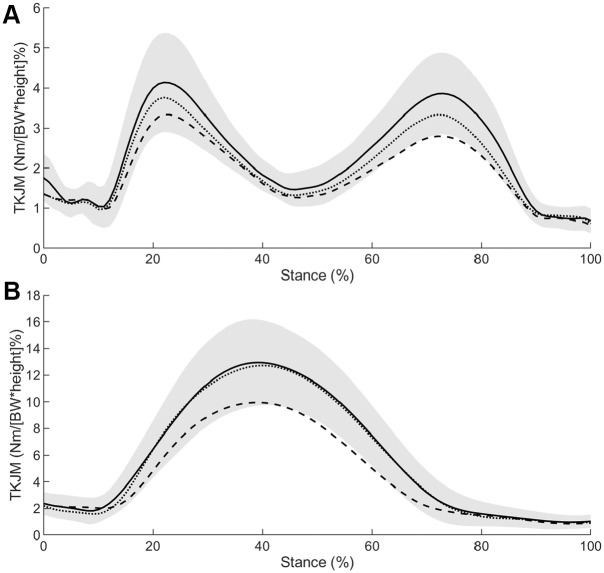
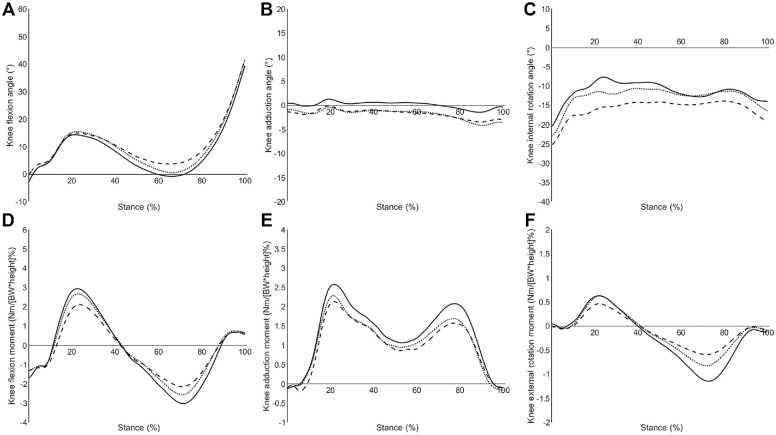
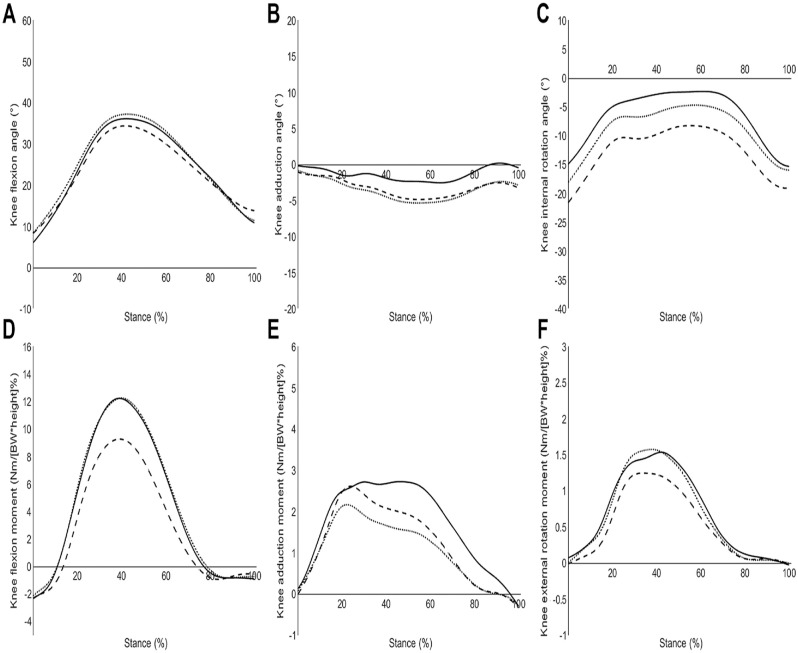
Methods: Kinematic and kinetic data were collected during running and walking in individuals after a meniscectomy and healthy individuals. Total knee joint moments (TKJM) were calculated from the sagittal, frontal, and transverse knee moments. Isometric quadriceps strength, perceived knee function, and kinesiophobia were also assessed. A mixed linear model compared differences between the affected leg, the contralateral leg, and the healthy leg.
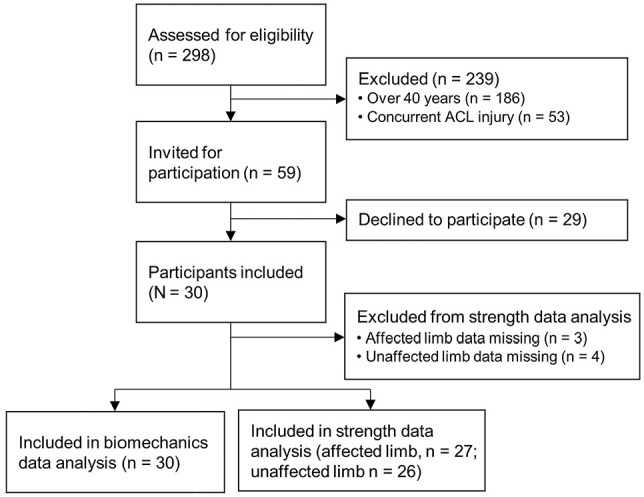
Results: Data were collected on 20 healthy individuals and 30 individuals after a meniscectomy (mean ± SD, 5.7 ± 2.9 months postsurgery), with 12, 16, and 2 individuals who had medial, lateral, and both medial and lateral meniscectomy, respectively. The affected limb demonstrated lower TKJM (P < .001), KFM (P = .004), and KRM (P < .001) during late stance of walking compared with the healthy group. Lower TKJM and KFM were observed during running in the affected limb compared with the contralateral limb and healthy group. No significant differences were observed between contralateral and healthy limbs except for KRM during late stance of walking. Lower quadriceps strength was observed in the affected (P < .001) and contralateral limbs (P = .001) compared with the healthy group. Individuals after a meniscectomy also reported greater kinesiophobia (P = .006) and lower perceived knee function (31.1%; P < .001) compared with the healthy group.
Conclusion: After meniscectomy, individuals who sustained a traumatic meniscal injury showed lower TKJM in the affected limb compared with the contralateral limb and healthy individuals. This decrease in TKJM can be attributed to altered knee-loading strategies in the sagittal and transverse planes.
Clinical relevance: Improving movement strategies, quadriceps strength, and kinesiophobia through rehabilitation approaches will allow individuals to load their knee appropriately when returning to sport.
Registration: NCT03379415 (ClinicalTrials.gov identifier).
Keywords: knee kinetics; meniscal injuries; running; total knee joint loading; walking.
© The Author(s) 2024.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from University of Salford (reference No. 18/EE/0015).
Figures
References
-
- Abram SGF, Price AJ, Judge A, Beard DJ. Anterior cruciate ligament (ACL) reconstruction and meniscal repair rates have both increased in the past 20 years in England: hospital statistics from 1997 to 2017. Br J Sports Med. 2020;54(5):286-291. - PubMed
-
- Andriacchi TP, Dyrby CO. Interactions between kinematics and loading during walking for the normal and ACL deficient knee. J Biomech. 2005;38(2):293-298. - PubMed
-
- Asay JL, Erhart-Hledik JC, Andriacchi TP. Changes in the total knee joint moment in patients with medial compartment knee osteoarthritis over 5 years. J Orthop Res. 2018;36(9):2373-2379. - PubMed
-
- Badlani JT, Borrero C, Golla S, Harner CD, Irrgang JJ. The effects of meniscus injury on the development of knee osteoarthritis: data from the osteoarthritis initiative. Am J Sports Med. 2013;41(6):1238-1244. - PubMed
-
- Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67:1-48.
Associated data
LinkOut - more resources
Full Text Sources
Medical
