

Laparoscopic or open abdominal surgery with thoracotomy for patients with oesophageal cancer: ROMIO randomized clinical trial
- PMID: 38525931
- PMCID: PMC10961947
- DOI: 10.1093/bjs/znae023
Laparoscopic or open abdominal surgery with thoracotomy for patients with oesophageal cancer: ROMIO randomized clinical trial
Abstract
Objective: This study investigated if hybrid oesophagectomy with minimally invasive gastric mobilization and thoracotomy enabled faster recovery than open surgery.
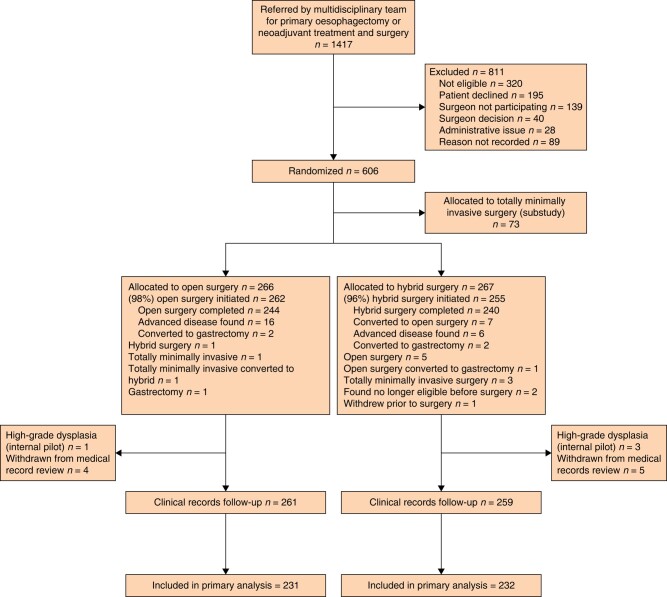
Methods: In eight UK centres, this pragmatic RCT recruited patients for oesophagectomy to treat localized cancer. Participants were randomly allocated to hybrid or open surgery, stratified by centre and receipt of neoadjuvant treatment. Large dressings aimed to mask patients to their allocation for six days post-surgery. The authors present the intention-to-treat analysis of outcome measures from the first 3 months post-randomization, including the primary outcome, the patient-reported physical function scale of the EORTC QLQ-C30, and cost-effectiveness. Current Controlled Trials registration: ISRCTN 59036820 (feasibility study), 10386621 (definitive study).
Findings: There was no evidence of a difference between hybrid (n = 267) and open (n = 266) surgery in average physical function over 3 months post-randomization: difference in means 2.1, 95% c.i. -2.0 to 6.2, P = 0.3. Complication rates were similar; for example, 88 (34%) participants in the open and 82 (32%) participants in the hybrid surgery groups experienced a pulmonary infection within 30 days. There was no evidence that hybrid surgery was more cost-effective than open surgery at 3 months.
Conclusions: Patient-reported physical function in the 3 months post-randomization provided no evidence of a difference in recovery time between hybrid and open surgery, or a difference in cost-effectiveness. Both approaches to surgery were completed safely, with a similar risk of key complications, suggesting that surgeons who have a preference for one of the two approaches need not change their practice.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Comment in
-
Advancing surgical options in esophageal cancer: key findings from the ROMIO randomized clinical trial.J Thorac Dis. 2025 Jan 24;17(1):5-9. doi: 10.21037/jtd-24-1803. Epub 2025 Jan 20. J Thorac Dis. 2025. PMID: 39975749 Free PMC article. No abstract available.
-
Laparoscopic or open abdominal surgery with thoracotomy: future directions from the ROMIO trial in esophageal cancer.J Thorac Dis. 2025 Feb 28;17(2):538-541. doi: 10.21037/jtd-24-1927. Epub 2025 Feb 27. J Thorac Dis. 2025. PMID: 40083509 Free PMC article. No abstract available.
-
Summary of the ROMIO randomized-control trial comparing clinical, economic and patient-reported outcomes between open versus hybrid esophagectomy in the United Kingdom.J Thorac Dis. 2025 Mar 31;17(3):1777-1783. doi: 10.21037/jtd-24-1862. Epub 2025 Mar 27. J Thorac Dis. 2025. PMID: 40223996 Free PMC article. No abstract available.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249 - PubMed
-
- Cromwell D, Wahedally H, Park MH, Maynard N, Crosby T, Trudgill N et al. National Oesophago-Gastric Cancer Audit 2019. London: Royal College of Surgeons of England, 2019
-
- Park MH, Wahedally MAH, Maynard N, Crosby T, Thomas B, Trudgill N et al. National Oesophago-Gastric Cancer Audit. 2022 Annual Report. London: The Royal College of Surgeons of England, 2023
-
- Nuytens F, Lenne X, Clement G, Bruandet A, Eveno C, Piessen G. Effect of phased implementation of totally minimally invasive Ivor Lewis esophagectomy for esophageal cancer after previous adoption of the hybrid minimally invasive technique: results from a French nationwide population-based cohort study. Ann Surg Oncol 2022;29:2791–2801 - PubMed
-
- Lagergren P, Avery KN, Hughes R, Barham CP, Alderson D, Falk SJ et al. Health-related quality of life among patients cured by surgery for esophageal cancer. Cancer 2007;110:686–693 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
