

Tungsten-Based Contrast Agent for Photon-Counting Detector CT Angiography in Calcified Coronaries: Comparison to Iodine in a Cardiovascular Phantom
- PMID: 38526041
- PMCID: PMC11827686
- DOI: 10.1097/RLI.0000000000001073
Tungsten-Based Contrast Agent for Photon-Counting Detector CT Angiography in Calcified Coronaries: Comparison to Iodine in a Cardiovascular Phantom
Abstract
Objectives: Calcified plaques induce blooming artifacts in coronary computed tomography angiography (CCTA) potentially leading to inaccurate stenosis evaluation. Tungsten represents a high atomic number, experimental contrast agent with different physical properties than iodine. We explored the potential of a tungsten-based contrast agent for photon-counting detector (PCD) CCTA in heavily calcified coronary vessels.
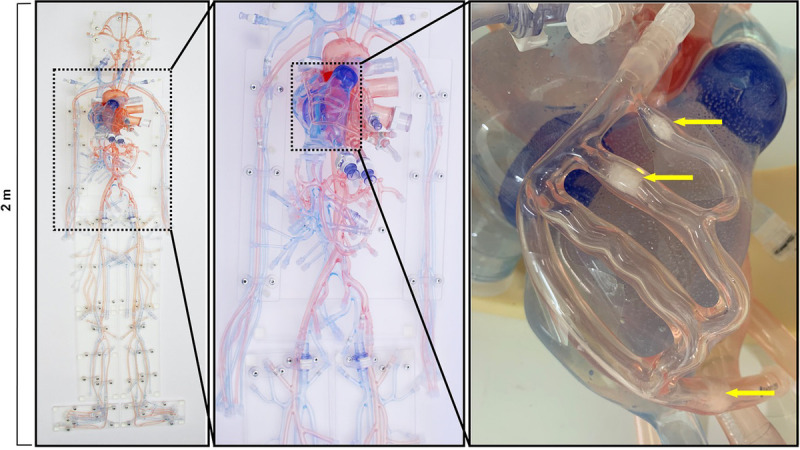
Materials and methods: A cardiovascular phantom exhibiting coronaries with calcified plaques was imaged on a first-generation dual-source PCD-CT. The coronaries with 3 different calcified plaques were filled with iodine and tungsten contrast media solutions equating to iodine and tungsten delivery rates (IDR and TDR) of 0.3, 0.5, 0.7, 1.0, 1.5, 2.0, 2.5, and 3.0 g/s, respectively. Electrocardiogram-triggered sequential acquisitions were performed in the spectral mode (QuantumPlus). Virtual monoenergetic images (VMIs) were reconstructed from 40 to 190 keV in 1 keV increments. Blooming artifacts and percentage error stenoses from calcified plaques were quantified, and attenuation characteristics of both contrast media were recorded.
Results: Blooming artifacts from calcified plaques were most pronounced at 40 keV (78%) and least pronounced at 190 keV (58%). Similarly, percentage error stenoses were highest at 40 keV (48%) and lowest at 190 keV (2%), respectively. Attenuation of iodine decreased monotonically in VMIs from low to high keV, with the strongest decrease from 40 keV to 100 keV (IDR of 2.5 g/s: 1279 HU at 40 keV, 187 HU at 100 kV, and 35 HU at 190 keV). The attenuation of tungsten, on the other hand, increased monotonically as a function of VMI energy, with the strongest increase between 40 and 100 keV (TDR of 2.5 g/s: 202 HU at 40 keV, 661 HU at 100 kV, and 717 HU at 190 keV). For each keV level, the relationship between attenuation and IDR/TDR could be described by linear regressions ( R2 ≥ 0.88, P < 0.001). Specifically, attenuation increased linearly when increasing the delivery rate irrespective of keV level or contrast medium. Iodine exhibited the highest relative increase in attenuation values at lower keV levels when increasing the IDR. Conversely, for tungsten, the greatest relative increase in attenuation values occurred at higher keV levels when increasing the TDR. When high keV imaging is desirable to reduce blooming artifacts from calcified plaques, IDR has to be increased at higher keV levels to maintain diagnostic vessel attenuation (ie, 300 HU), whereas for tungsten, TDR can be kept constant or can be even reduced at high keV energy levels.
Conclusions: Tungsten's attenuation characteristics in relation to VMI energy levels are reversed to those of iodine, with tungsten exhibiting high attenuation values at high keV levels and vice versa. Thus, tungsten shows promise for high keV imaging CCTA with PCD-CT as-in distinction to iodine-both high vessel attenuation and low blooming artifacts from calcified plaques can be achieved.
Copyright © 2024 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest and sources of funding: M.C.M., G.J., and H.P. are employees of Bayer AG. R.G., T.N., B.S., and T.G.F. are employees of Siemens Healthineers. J.E.W. received institutional grants via Clinical Trial Center Maastricht from Bard, Bayer, Boston, Brainlab, GE, Philips, Siemens, as well as speaker's bureau via Maastricht UMC+ from Bayer and Siemens. H.A. received institutional grants from Bayer, Guerbet, Canon, and Siemens, as well as speaker's bureau from Siemens.
Figures





Similar articles
-
High-Pitch Multienergy Coronary CT Angiography in Dual-Source Photon-Counting Detector CT Scanner at Low Iodinated Contrast Dose.Invest Radiol. 2023 Sep 1;58(9):681-690. doi: 10.1097/RLI.0000000000000961. Invest Radiol. 2023. PMID: 36822655 Free PMC article.
-
Countering Calcium Blooming With Personalized Contrast Media Injection Protocols: The 1-2-3 Rule for Photon-Counting Detector CCTA.Invest Radiol. 2024 Oct 1;59(10):684-690. doi: 10.1097/RLI.0000000000001078. Epub 2024 May 15. Invest Radiol. 2024. PMID: 38742928 Free PMC article.
-
Photon-Counting Detector CT: Clinical Utility of Virtual Monoenergetic Imaging Combined With Tin Prefiltration to Reduce Metal Artifacts in the Postoperative Ankle.Invest Radiol. 2024 Aug 1;59(8):545-553. doi: 10.1097/RLI.0000000000001058. Epub 2024 Jan 10. Invest Radiol. 2024. PMID: 38214560
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
Cited by
-
Photon-Counting CT: Technology, Current and Potential Future Clinical Applications, and Overview of Approved Systems and Those in Various Stages of Research and Development.Radiology. 2025 Mar;314(3):e240662. doi: 10.1148/radiol.240662. Radiology. 2025. PMID: 40067107 Review.
-
Insights into nanoparticle surface bonding and coating architecture via multinuclear NMR.Acad Nano. 2025;2(2):7737. doi: 10.20935/acadnano7737. Epub 2025 May 29. Acad Nano. 2025. PMID: 40575764 Free PMC article.
-
An Image-Based Prior Knowledge-Free Approach for a Multi-Material Decomposition in Photon-Counting Computed Tomography.Diagnostics (Basel). 2024 Jun 14;14(12):1262. doi: 10.3390/diagnostics14121262. Diagnostics (Basel). 2024. PMID: 38928677 Free PMC article.
-
K-Edge Imaging Using a Clinical Dual-Source Photon-Counting CT System.medRxiv [Preprint]. 2025 Aug 24:2025.08.21.25333798. doi: 10.1101/2025.08.21.25333798. medRxiv. 2025. PMID: 40894147 Free PMC article. Preprint.
References
-
- Knuuti J Wijns W Saraste A, et al. . 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–477. - PubMed
-
- Van Hedent S Große Hokamp N Kessner R, et al. . Effect of virtual monoenergetic images from spectral detector computed tomography on coronary calcium blooming. J Comput Assist Tomogr. 2018;42:912–918. - PubMed
-
- Secchi F De Cecco CN Spearman JV, et al. . Monoenergetic extrapolation of cardiac dual energy CT for artifact reduction. Acta Radiol. 2015;56:413–418. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
