

Inappropriate Diagnosis of Pneumonia Among Hospitalized Adults
- PMID: 38526476
- PMCID: PMC10964165
- DOI: 10.1001/jamainternmed.2024.0077
Inappropriate Diagnosis of Pneumonia Among Hospitalized Adults
Abstract
Importance: Little is known about incidence of, risk factors for, and harms associated with inappropriate diagnosis of community-acquired pneumonia (CAP).
Objective: To characterize inappropriate diagnosis of CAP in hospitalized patients.
Design, setting, and participants: This prospective cohort study, including medical record review and patient telephone calls, took place across 48 Michigan hospitals. Trained abstractors retrospectively assessed hospitalized patients treated for CAP between July 1, 2017, and March 31, 2020. Patients were eligible for inclusion if they were adults admitted to general care with a discharge diagnostic code of pneumonia who received antibiotics on day 1 or 2 of hospitalization. Data were analyzed from February to December 2023.
Main outcomes and measures: Inappropriate diagnosis of CAP was defined using a National Quality Forum-endorsed metric as CAP-directed antibiotic therapy in patients with fewer than 2 signs or symptoms of CAP or negative chest imaging. Risk factors for inappropriate diagnosis were assessed and, for those inappropriately diagnosed, 30-day composite outcomes (mortality, readmission, emergency department visit, Clostridioides difficile infection, and antibiotic-associated adverse events) were documented and stratified by full course (>3 days) vs brief (≤3 days) antibiotic treatment using generalized estimating equation models adjusting for confounders and propensity for treatment.
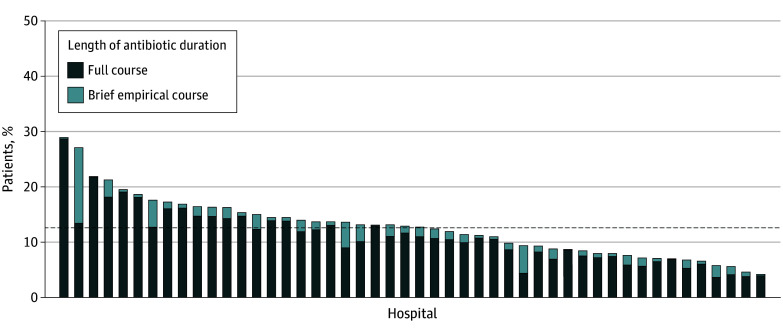
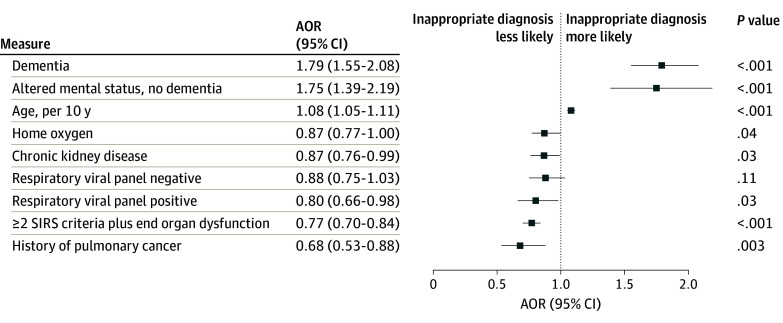
Results: Of the 17 290 hospitalized patients treated for CAP, 2079 (12.0%) met criteria for inappropriate diagnosis (median [IQR] age, 71.8 [60.1-82.8] years; 1045 [50.3%] female), of whom 1821 (87.6%) received full antibiotic courses. Compared with patients with CAP, patients inappropriately diagnosed were older (adjusted odds ratio [AOR], 1.08; 95% CI, 1.05-1.11 per decade) and more likely to have dementia (AOR, 1.79; 95% CI, 1.55-2.08) or altered mental status on presentation (AOR, 1.75; 95% CI, 1.39-2.19). Among those inappropriately diagnosed, 30-day composite outcomes for full vs brief treatment did not differ (25.8% vs 25.6%; AOR, 0.98; 95% CI, 0.79-1.23). Full vs brief duration of antibiotic treatment among patients was associated with antibiotic-associated adverse events (31 of 1821 [2.1%] vs 1 of 258 [0.4%]; P = .03).
Conclusions and relevance: In this cohort study, inappropriate diagnosis of CAP among hospitalized adults was common, particularly among older adults, those with dementia, and those presenting with altered mental status. Full-course antibiotic treatment of those inappropriately diagnosed with CAP may be harmful.
Conflict of interest statement
Figures
References
-
- McDermott KW, Roemer M. Most frequent principal diagnoses for inpatient stays in US hospitals, 2018. Healthcare Cost and Utilization Project . July 13, 2021. Accessed December 8, 2022. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb277-Top-Reasons-Hospit... - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
