

Pharmacologic prevention and therapy of postoperative paralytic ileus after gastrointestinal cancer surgery: systematic review and meta-analysis
- PMID: 38526522
- PMCID: PMC11254286
- DOI: 10.1097/JS9.0000000000001393
Pharmacologic prevention and therapy of postoperative paralytic ileus after gastrointestinal cancer surgery: systematic review and meta-analysis
Abstract
Background: Postoperative paralytic ileus (POI) is a significant concern following gastrointestinal tumor surgery. Effective preventive and therapeutic strategies are crucial but remain elusive. Current evidence from randomized-controlled trials on pharmacological interventions for prevention or treatment of POI are systematically reviewed to guide clinical practice and future research.
Materials and methods: Literature was systematically searched for prospective randomized-controlled trials testing pharmacological interventions for prevention or treatment of POI after gastrointestinal tumor surgery. Meta-analysis was performed using a random effects model to determine risk ratios and mean differences with 95% CI. Risk of bias and evidence quality were assessed.
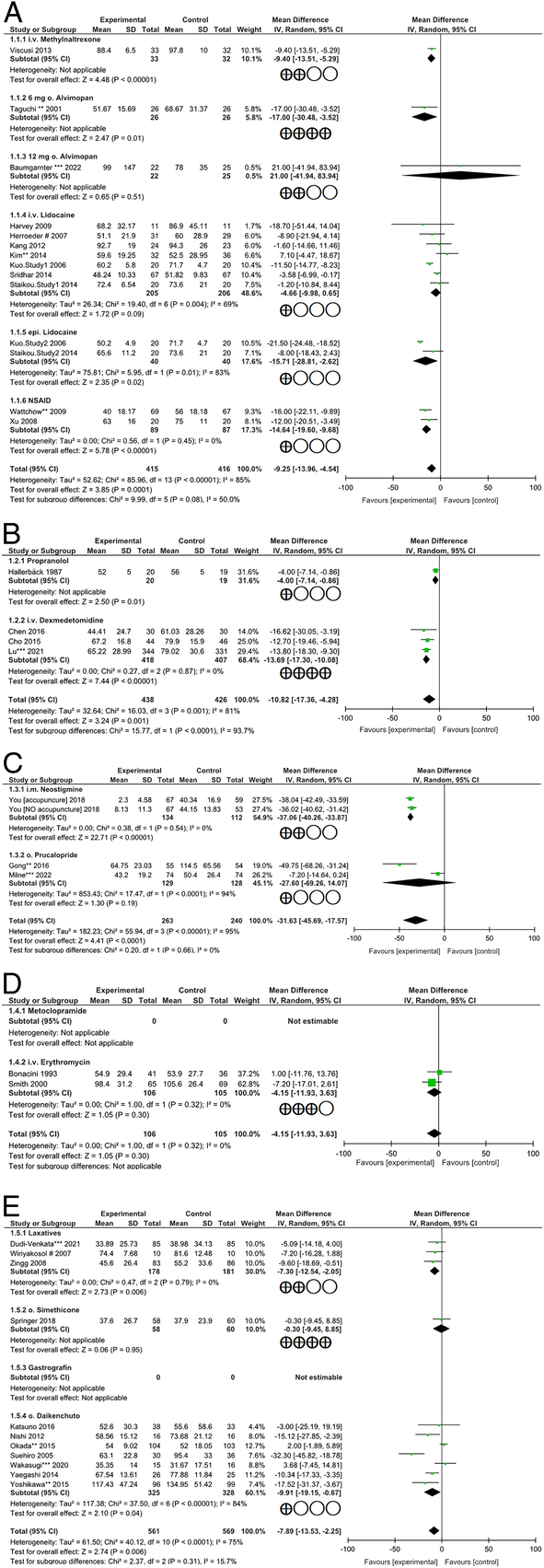
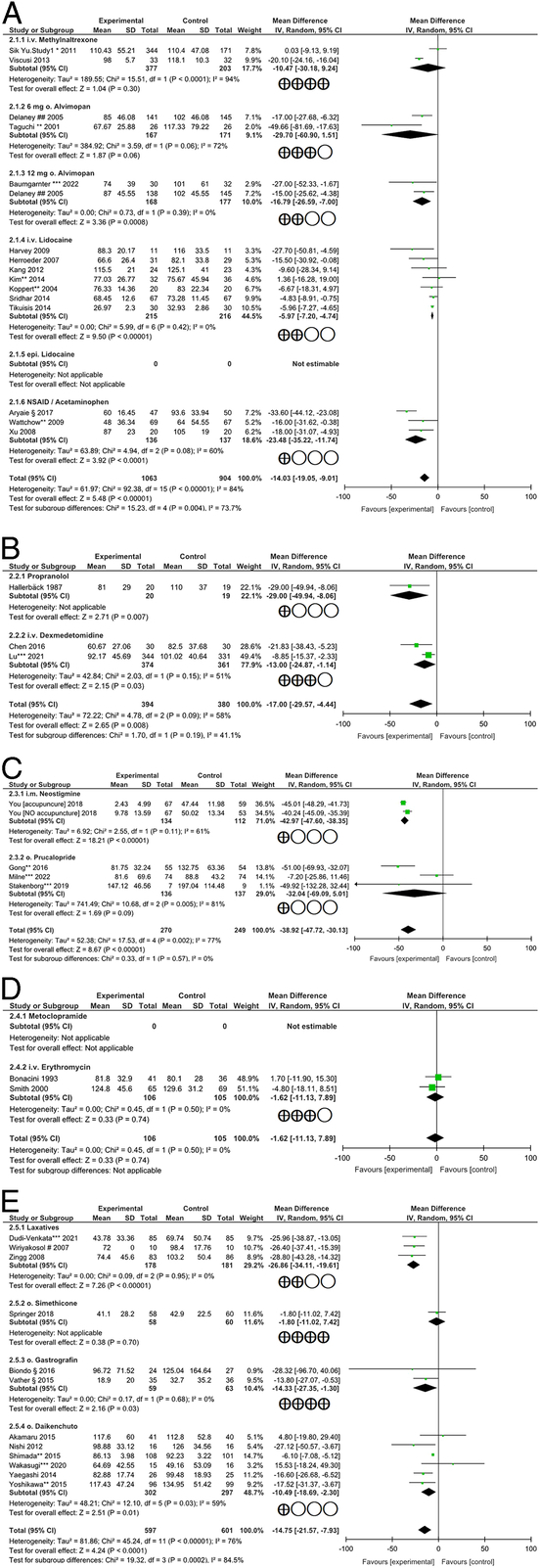
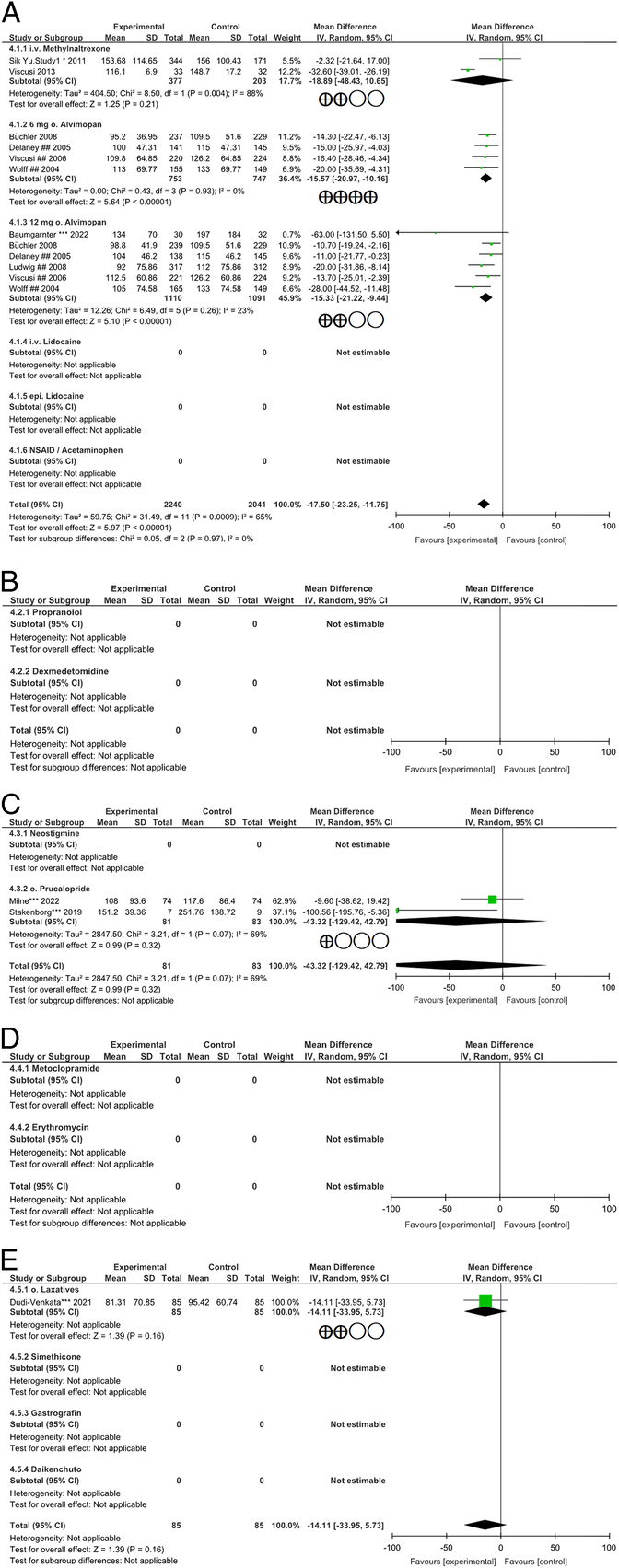
Results: Results from 55 studies, involving 5078 patients who received experimental interventions, indicate that approaches of opioid-sparing analgesia, peripheral opioid antagonism, reduction of sympathetic hyperreactivity, and early use of laxatives effectively prevent POI. Perioperative oral Alvimopan or intravenous administration of Lidocaine or Dexmedetomidine, while safe regarding cardio-pulmonary complications, demonstrated effectiveness concerning various aspects of postoperative bowel recovery [Lidocaine: -5.97 (-7.20 to -4.74)h, P <0.0001; Dexmedetomidine: -13.00 (-24.87 to -1.14)h, P =0.03 for time to first defecation; Alvimopan: -15.33 (-21.22 to -9.44)h, P <0.0001 for time to GI-2 ] and length of hospitalization [Lidocaine: -0.67 (-1.24 to -0.09)d, P =0.02; Dexmedetomidine: -1.28 (-1.96 to -0.60)d, P =0.0002; Alvimopan: -0.58 (-0.84 to -0.32)d, P <0.0001] across wide ranges of evidence quality. Perioperative nonopioid analgesic use showed efficacy concerning bowel recovery as well as length of hospitalization [-1.29 (-1.95 to -0.62)d, P =0.0001]. Laxatives showed efficacy regarding bowel movements, but not food tolerance and hospitalization. Evidence supporting pharmacological treatment for clinically evident POI is limited. Results from one single study suggest that Neostigmine reduces time to flatus and accelerates bowel movements [-37.06 (-40.26 to -33.87)h, P <0.0001 and -42.97 (-47.60 to -38.35)h, P <0.0001, respectively] with low evidence quality.
Conclusion: Current evidence concerning pharmacological prevention and treatment of POI following gastrointestinal tumor surgery is limited. Opioid-sparing concepts, reduction of sympathetic hyperreactivity, and laxatives should be implemented into multimodal perioperative approaches.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
No conflicts of interests to be declared concerning this article.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures


References
-
- Milne TGE, Jaung R, O’Grady G, et al. Nonsteroidal anti-inflammatory drugs reduce the time to recovery of gut function after elective colorectal surgery: a systematic review and meta-analysis. Colorectal Dis 2018;20:O190–O198. - PubMed
-
- Traeger L, Kroon HM, Bedrikovetski S, et al. The impact of acetylcholinesterase inhibitors on ileus and gut motility following abdominal surgery: a clinical review. ANZ J Surg 2022;92:69–76. - PubMed
-
- Reichert M, Weber C, Pons-Kuhnemann J, et al. Protective loop ileostomy increases the risk for prolonged postoperative paralytic ileus after open oncologic rectal resection. Int J Colorectal Dis 2018;33:1551–1557. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
