

Deep Learning to Estimate Cardiovascular Risk From Chest Radiographs : A Risk Prediction Study
- PMID: 38527287
- PMCID: PMC11613935
- DOI: 10.7326/M23-1898
Deep Learning to Estimate Cardiovascular Risk From Chest Radiographs : A Risk Prediction Study
Erratum in
-
Correction: Deep Learning to Estimate Cardiovascular Risk From Chest Radiographs.Ann Intern Med. 2025 Jan;178(1):147. doi: 10.7326/ANNALS-24-03386. Epub 2024 Dec 17. Ann Intern Med. 2025. PMID: 39680924 No abstract available.
Abstract
Background: Guidelines for primary prevention of atherosclerotic cardiovascular disease (ASCVD) recommend a risk calculator (ASCVD risk score) to estimate 10-year risk for major adverse cardiovascular events (MACE). Because the necessary inputs are often missing, complementary approaches for opportunistic risk assessment are desirable.
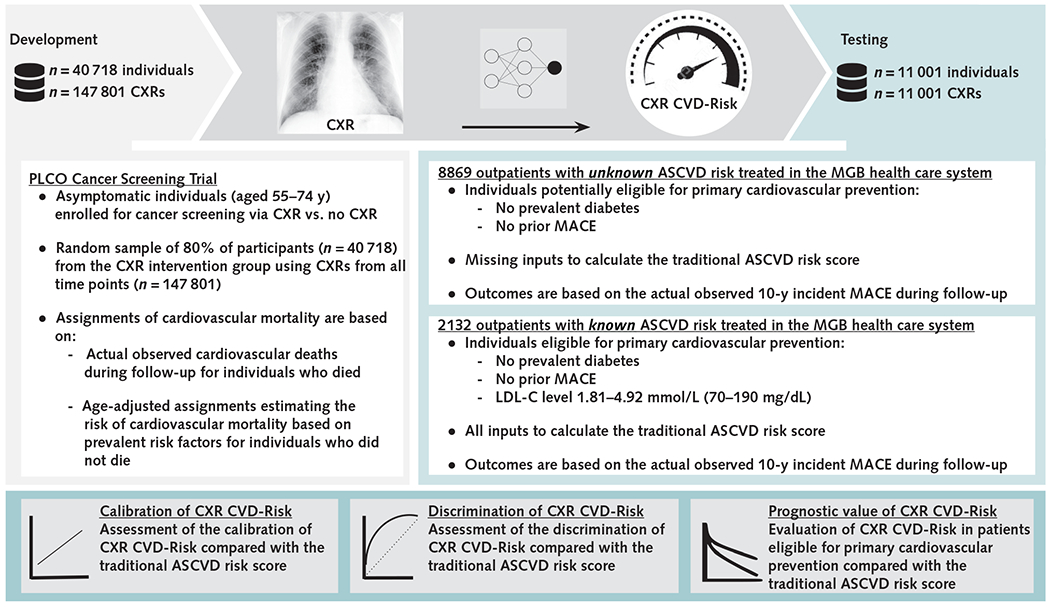
Objective: To develop and test a deep-learning model (CXR CVD-Risk) that estimates 10-year risk for MACE from a routine chest radiograph (CXR) and compare its performance with that of the traditional ASCVD risk score for implications for statin eligibility.
Design: Risk prediction study.
Setting: Outpatients potentially eligible for primary cardiovascular prevention.
Participants: The CXR CVD-Risk model was developed using data from a cancer screening trial. It was externally validated in 8869 outpatients with unknown ASCVD risk because of missing inputs to calculate the ASCVD risk score and in 2132 outpatients with known risk whose ASCVD risk score could be calculated.
Measurements: 10-year MACE predicted by CXR CVD-Risk versus the ASCVD risk score.
Results: Among 8869 outpatients with unknown ASCVD risk, those with a risk of 7.5% or higher as predicted by CXR CVD-Risk had higher 10-year risk for MACE after adjustment for risk factors (adjusted hazard ratio [HR], 1.73 [95% CI, 1.47 to 2.03]). In the additional 2132 outpatients with known ASCVD risk, CXR CVD-Risk predicted MACE beyond the traditional ASCVD risk score (adjusted HR, 1.88 [CI, 1.24 to 2.85]).
Limitation: Retrospective study design using electronic medical records.
Conclusion: On the basis of a single CXR, CXR CVD-Risk predicts 10-year MACE beyond the clinical standard and may help identify individuals at high risk whose ASCVD risk score cannot be calculated because of missing data.
Primary funding source: None.
Conflict of interest statement
Figures


References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al.; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2023 update: a report from the American Heart Association. Circulation. 2023;147:e93–e621. doi:10.1161/CIR.0000000000001123 - DOI - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;73:3168–3209. doi:10.1016/j.jacc.2018.11.002 - DOI - PubMed
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2935–2959. doi:10.1016/j.jacc.2013.11.005 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical