

Acute kidney injury in patients with cirrhosis: Acute Disease Quality Initiative (ADQI) and International Club of Ascites (ICA) joint multidisciplinary consensus meeting
- PMID: 38527522
- PMCID: PMC11193657
- DOI: 10.1016/j.jhep.2024.03.031
Acute kidney injury in patients with cirrhosis: Acute Disease Quality Initiative (ADQI) and International Club of Ascites (ICA) joint multidisciplinary consensus meeting
Abstract
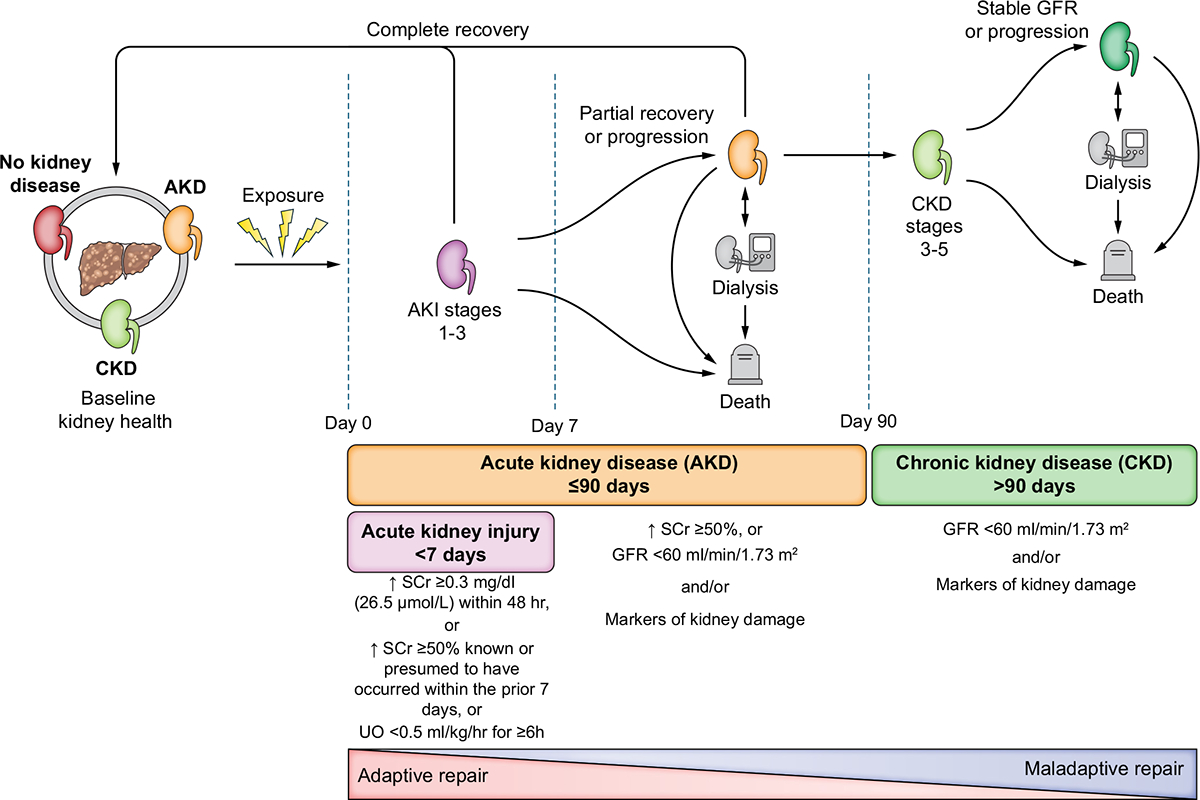
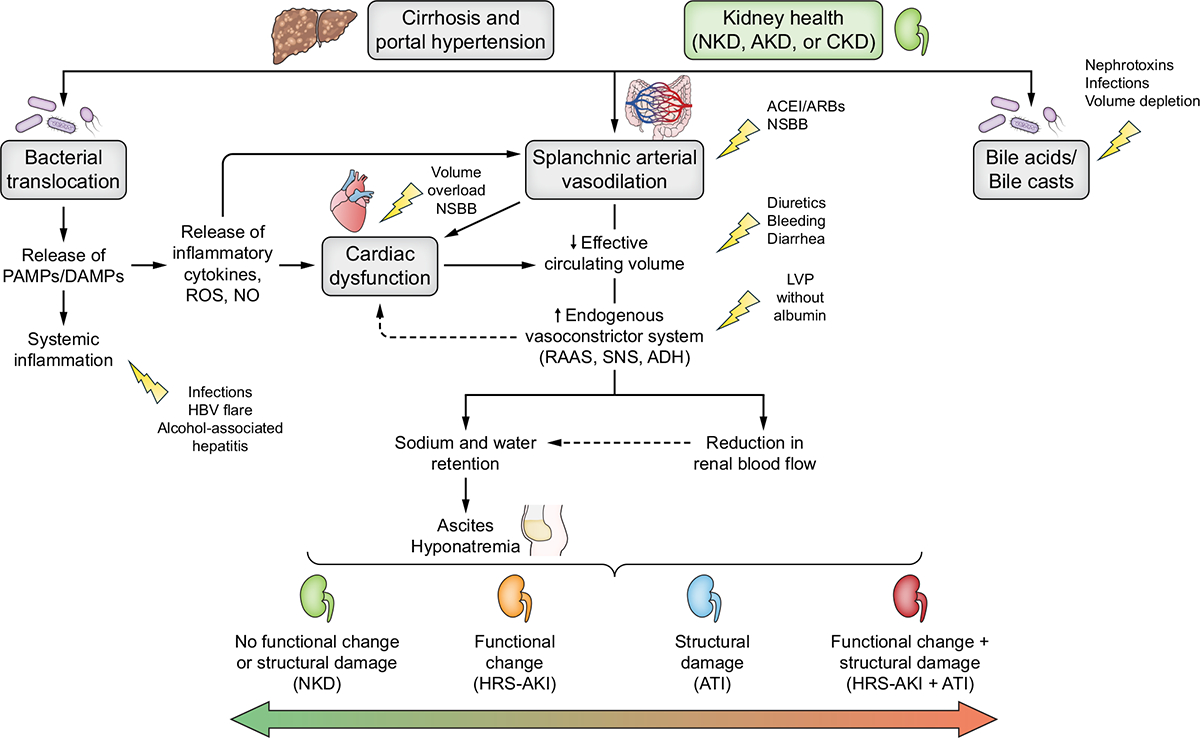
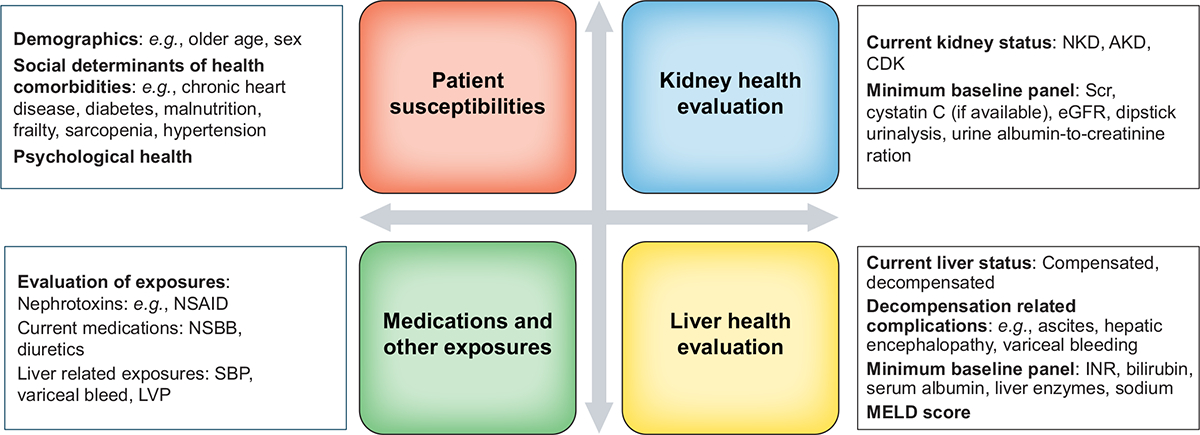
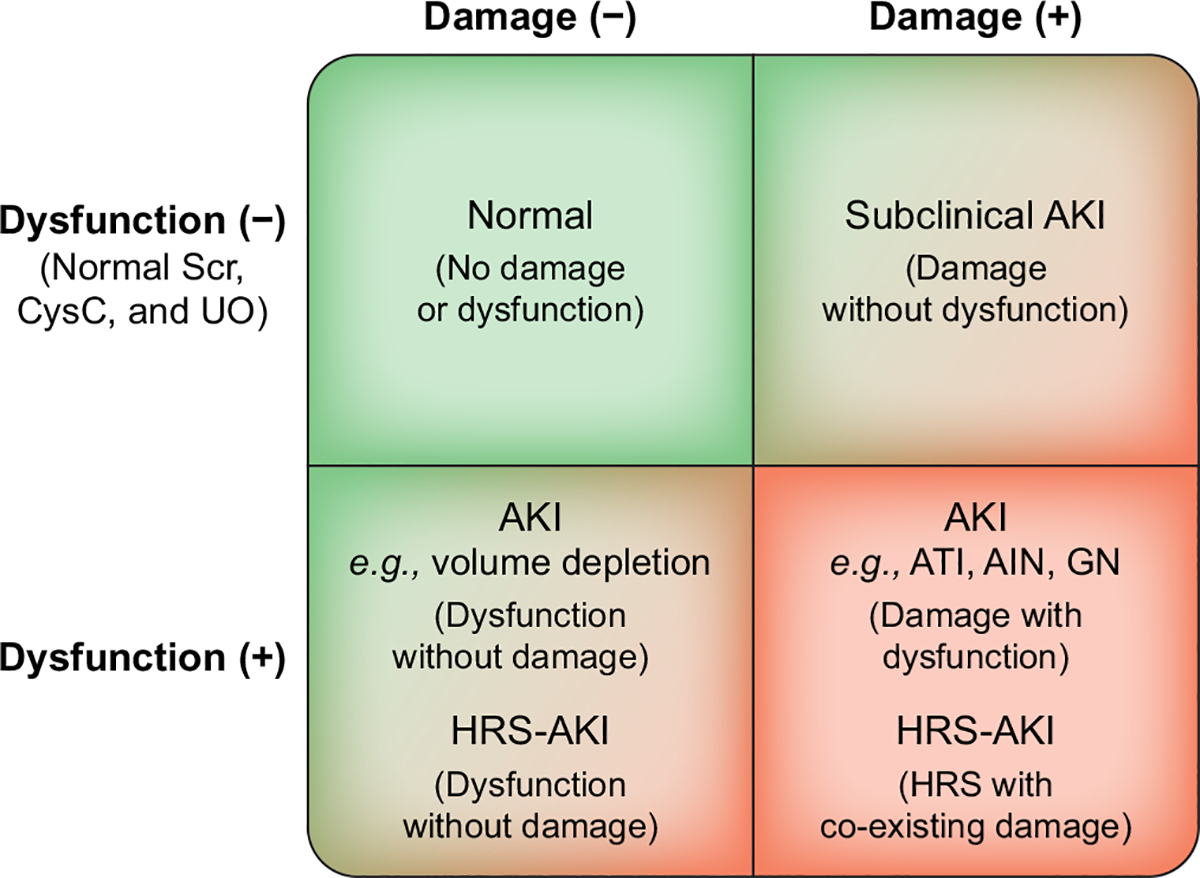
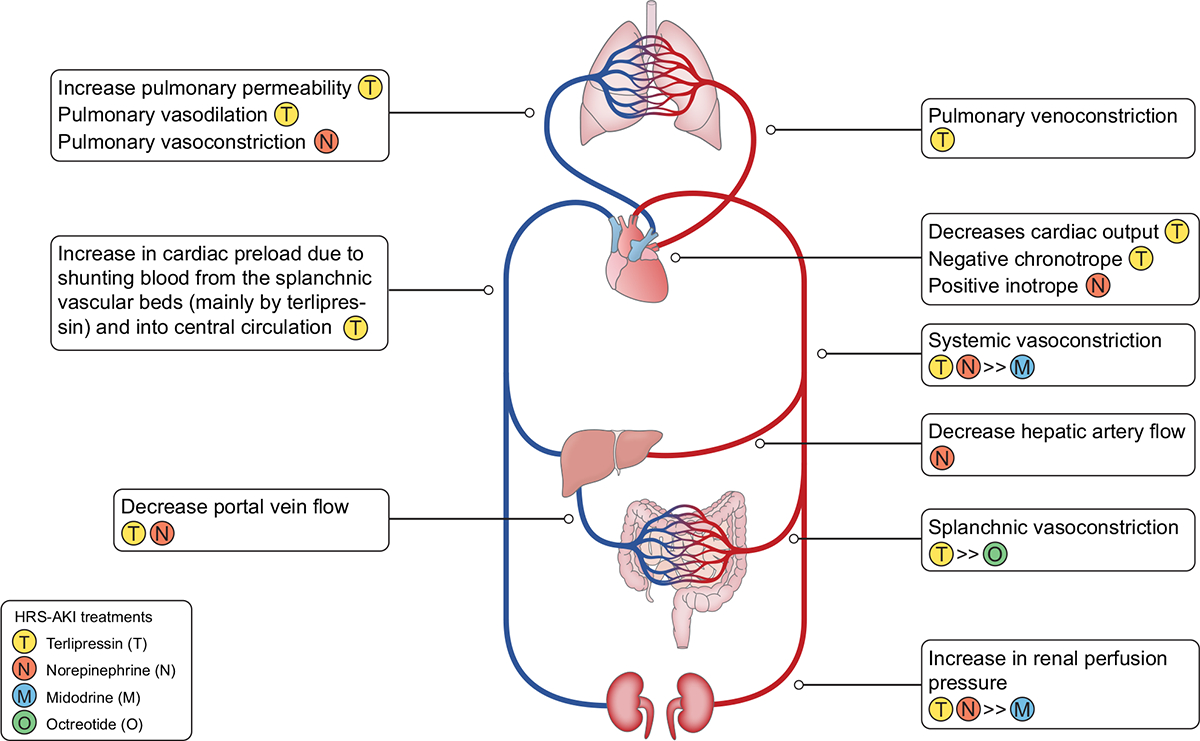
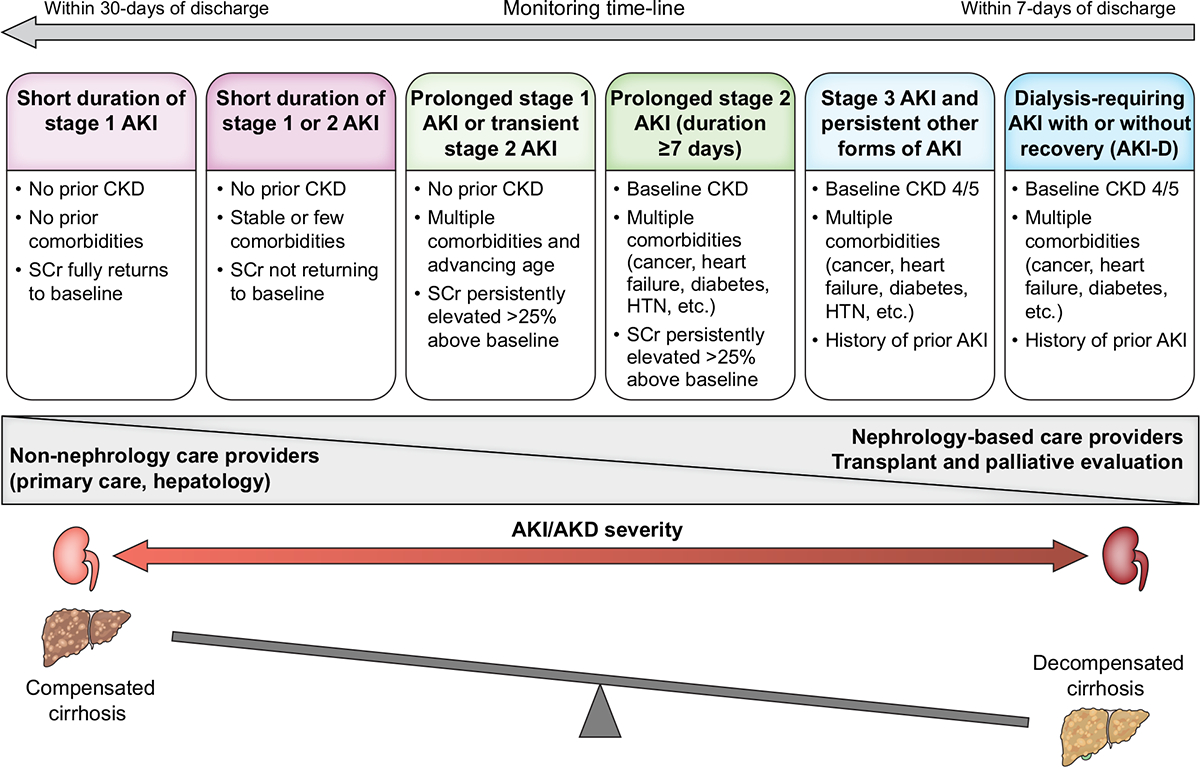
Patients with cirrhosis are prone to developing acute kidney injury (AKI), a complication associated with a markedly increased in-hospital morbidity and mortality, along with a risk of progression to chronic kidney disease. Whereas patients with cirrhosis are at increased risk of developing any phenotype of AKI, hepatorenal syndrome (HRS), a specific form of AKI (HRS-AKI) in patients with advanced cirrhosis and ascites, carries an especially high mortality risk. Early recognition of HRS-AKI is crucial since administration of splanchnic vasoconstrictors may reverse the AKI and serve as a bridge to liver transplantation, the only curative option. In 2023, a joint meeting of the International Club of Ascites (ICA) and the Acute Disease Quality Initiative (ADQI) was convened to develop new diagnostic criteria for HRS-AKI, to provide graded recommendations for the work-up, management and post-discharge follow-up of patients with cirrhosis and AKI, and to highlight priorities for further research.
Keywords: acute disease quality initiative; acute kidney injury; albumin; ascites; biomarker; cirrhosis; hepatorenal syndrome; international club of ascites; liver transplantation; renal replacement therapy; terlipressin.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
MKN has received consulting/advisory board fees from Mallinckrodt Pharmaceuticals, Ocelot and Baxter; JAK has received grant support and consulting fees from Astute Medical/BioMerieux, Novaratis; Fulltime employee, Spectral Medical; LF has received research support from Baxter and Ortho Clinical Diagnostics; MO has received research funding from Baxter, Biomerieux and La Jolla Pharma; ASA has received consulting/advisory board fees from Mallinckrodt Pharmaceuticals and Ocelot; JAN has received consulting fees from Baxter, Outset Medical, and Vifor Pharma; JCO has received consulting fees from Mallinckrodt Pharmaceuticals; SP has received consulting fees from Plasma Protein Therapeutics association, advisory board fees from Mallinckrodt Pharmaceuticals and speaking fees from Grifols and Medscape; LBV has received research support from W.L. Gore & Associates; ECV has received research support to institution from Salix; AAA’s institution has received research funding from Baxter, Bioporto, and Medtronic; PA has received advisory board fees from Biovie, Biomarin, and speaking fees from Grifols, CSL Bhering and Kedrion; JMB has received consulting/advisory board fees from Mallinckrodt; PG has received research funding from Gilead & Grifols, has consulted or attended advisory boards for Gilead, RallyBio, SeaBeLife, Merck, Sharp and Dohme (MSD), Ocelot Bio and Behring, and received speaking fees from Pfizer; MK has received speaker fees from Baxter, Fresenius Medical Care and B.Braun; CR has been consultant or member of advisory board and/or Speaker Bureau for Asahi medical, Aferetica, Baxter, B.Braun, Biomerieux, Cytosorbents, Fresenoius mecial care, Medtronic, ESTOR, Medica, Jafron, OCD, GE, Toray, Nipro, Sphingotec; JCV has received honoraria from Mallinckrodt Pharmaceuticals (consulting, speaking bureau), Travere Therapeutics (advisory) and Calliditas (advisory); RLM has received consulting/advisory board fees from Baxter, Fresenius, AM Pharma, Alexion, Unicycive, Guard, Novartis, Renibus, Mallinckrodt and Sphingotec; FD has received consulting/advisory board fees from Chiesi and Biotest; CF, SA, SWB, AD, YSG, PSK, SKG, NL, EM, RM, SM, RHP, PT have nothing to declare.
Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
