

Predicting factors for acute encephalopathy in febrile seizure children with SARS-CoV-2 omicron variant: a retrospective study
- PMID: 38528535
- PMCID: PMC10962131
- DOI: 10.1186/s12887-024-04699-x
Predicting factors for acute encephalopathy in febrile seizure children with SARS-CoV-2 omicron variant: a retrospective study
Abstract
Background: SARS-CoV-2 posed a threat to children during the early phase of Omicron wave because many patients presented with febrile seizures. The study aimed to investigate predicting factors for acute encephalopathy of children infected by SARS-CoV-2 Omicron variant presenting with febrile seizures.
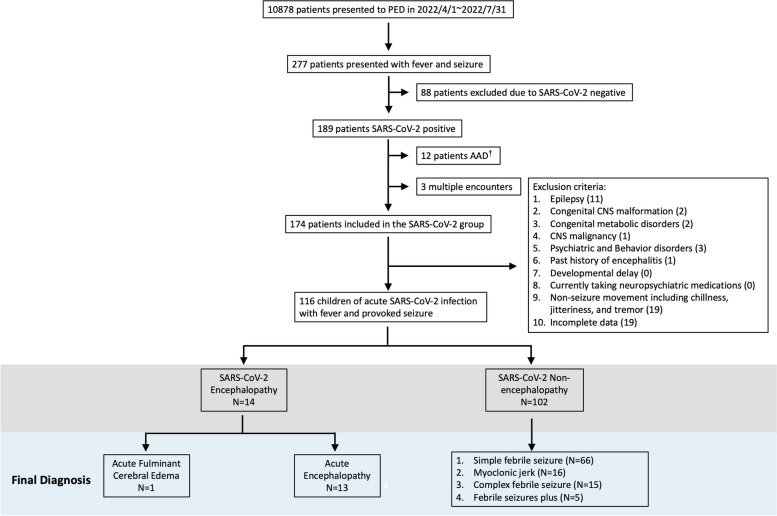
Methods: The retrospective study analyzed data from pediatric patients who visited the emergency department of Chang Gung Memorial Hospital in Taiwan between April and July 2022. We specifically focused on children with COVID-19 who presented with febrile seizures, collecting demographic, clinical, and laboratory data at the pediatric emergency department, as well as final discharge diagnoses. Subsequently, we conducted a comparative analysis of the clinical and laboratory characteristics between patients diagnosed with acute encephalopathy and those with other causes of febrile seizures.
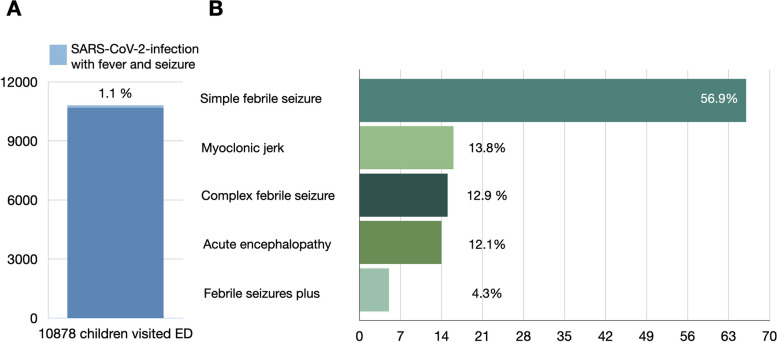
Results: Overall, 10,878 children were included, of which 260 patients presented with febrile seizures. Among them, 116 individuals tested positive for SARS-CoV-2 and of them, 14 subsequently developed acute encephalopathy (12%). Those with acute encephalopathy displayed distinctive features, including older age (5.1 vs. 2.6 years old), longer fever duration preceding the first seizure (1.6 vs. 0.9 days), cluster seizure (50% vs. 16.7%), status epilepticus (50% vs. 13.7%) and occurrences of bradycardia (26.8% vs. 0%) and hypotension (14.3% vs. 0%) in the encephalopathy group. Besides, the laboratory findings in the encephalopathy group are characterized by hyperglycemia (mean (95% CI) 146 mg/dL (95% CI 109-157) vs. 108 mg/dL (95% CI 103-114) and metabolic acidosis (mean (95% CI) pH 7.29(95% CI 7.22-7.36) vs. 7.39 (95%CI 7.37-7.41)).
Conclusions: In pediatric patients with COVID-19-related febrile seizures, the occurrence of seizures beyond the first day of fever, bradycardia, clustered seizures, status epilepticus, hyperglycemia, and metabolic acidosis should raise concerns about acute encephalitis/encephalopathy. However, the highest body temperature and the severity of leukocytosis or C-reactive protein levels were not associated with poor outcomes.
Keywords: COVID-19; Encephalopathy; Febrile seizures; Pediatric; Predictive factor; SARS-CoV-2.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Risk factors of Omicron variant associated acute encephalitis/encephalopathy in children.J Microbiol Immunol Infect. 2023 Dec;56(6):1169-1177. doi: 10.1016/j.jmii.2023.08.010. Epub 2023 Sep 4. J Microbiol Immunol Infect. 2023. PMID: 37709632
-
Evaluation of patients presenting with febrile seizures in an Iranian referral hospital: emphasis on the frequency of meningitis and co-infections.BMC Pediatr. 2023 Jun 22;23(1):316. doi: 10.1186/s12887-023-04120-z. BMC Pediatr. 2023. PMID: 37349740 Free PMC article.
-
The Impact of Omicron Wave on Pediatric Febrile Seizure.J Korean Med Sci. 2023 Jan 16;38(3):e18. doi: 10.3346/jkms.2023.38.e18. J Korean Med Sci. 2023. PMID: 36647218 Free PMC article.
-
A Systematic Review and Clinical Presentation of Central Nervous System Complications of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospitalized Pediatric Patients During the Coronavirus Disease 2019 Pandemic in Israel.Pediatr Neurol. 2024 Apr;153:68-76. doi: 10.1016/j.pediatrneurol.2024.01.008. Epub 2024 Jan 11. Pediatr Neurol. 2024. PMID: 38335916
-
Defining the Clinicoradiologic Syndrome of SARS-CoV-2 Acute Necrotizing Encephalopathy: A Systematic Review and 3 New Pediatric Cases.Neurol Neuroimmunol Neuroinflamm. 2024 Jan;11(1):e200186. doi: 10.1212/NXI.0000000000200186. Epub 2023 Dec 7. Neurol Neuroimmunol Neuroinflamm. 2024. PMID: 38086061 Free PMC article.
Cited by
-
Case report of brain death in a child due to COVID-19 and literature review.BMC Infect Dis. 2025 May 14;25(1):700. doi: 10.1186/s12879-025-11058-3. BMC Infect Dis. 2025. PMID: 40369424 Free PMC article. Review.
-
Identification of Genetic Variants in Status Epilepticus Associated With Fever.Brain Behav. 2025 Feb;15(2):e70279. doi: 10.1002/brb3.70279. Brain Behav. 2025. PMID: 39915231 Free PMC article.
References
-
- Chou SH, Beghi E, Helbok R, Moro E, Sampson J, Altamirano V, Mainali S, Bassetti C, Suarez JI, McNett M. Global incidence of neurological manifestations among patients hospitalized with COVID-19-A report for the GCS-NeuroCOVID consortium and the ENERGY consortium. JAMA Netw Open. 2021;4(5):e2112131. - PMC - PubMed
-
- Manzano GS, McEntire CRS, Martinez-Lage M, Mateen FJ, Hutto SK. Acute disseminated encephalomyelitis and acute hemorrhagic leukoencephalitis following COVID-19: systematic review and meta-synthesis. Neurol Neuroimmunol Neuroinflamm. 2021;8(6):e1080. doi: 10.1212/NXI.0000000000001080. - DOI - PMC - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
