

Enhancing Diabetic Macular Edema Treatment Outcomes: Exploring the ESASO Classification and Structural OCT Biomarkers
- PMID: 38530567
- PMCID: PMC11039609
- DOI: 10.1007/s40123-024-00925-y
Enhancing Diabetic Macular Edema Treatment Outcomes: Exploring the ESASO Classification and Structural OCT Biomarkers
Abstract
Introduction: This study assessed the European School of Advanced Studies in Ophthalmology (ESASO) classification's prognostic value for diabetic macular edema (DME) in predicting intravitreal therapy outcomes.
Methods: In this retrospective, multicenter study, patients aged > 50 years with type 1 or 2 diabetes and DME received intravitreal antivascular endothelial growth factor (anti-VEGF) agents (ranibizumab, bevacizumab, and aflibercept) or steroids (dexamethasone). The primary outcome was visual acuity (VA) change post-treatment, termed as functional response, measured 4-6 weeks post-third anti-VEGF or 12-16 weeks post-steroid injection, stratified by initial DME stage.
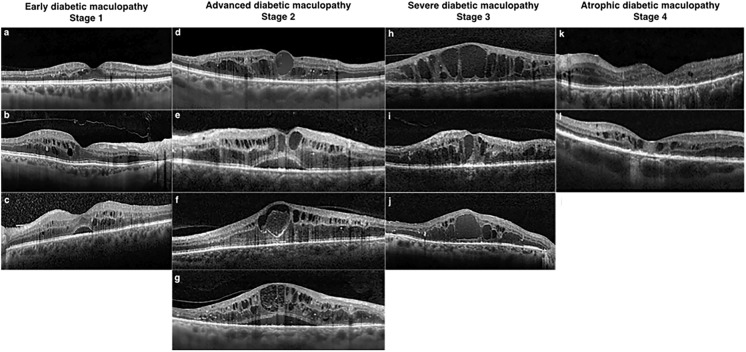
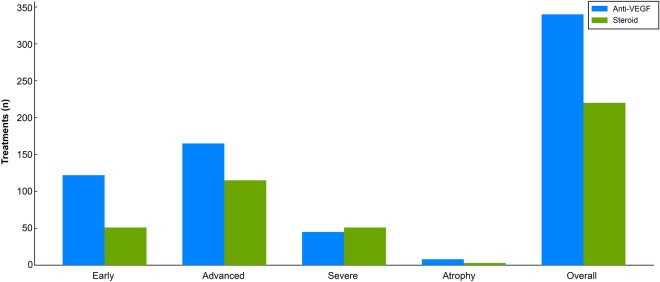
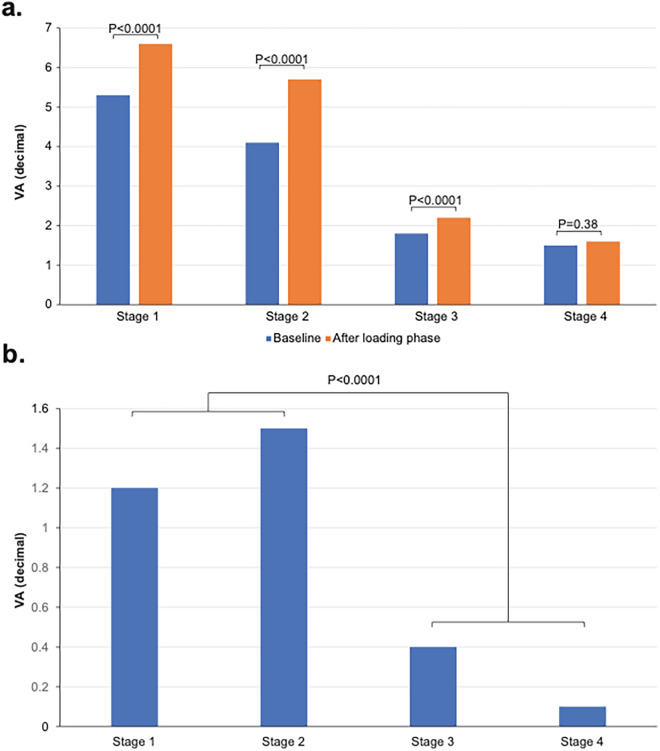
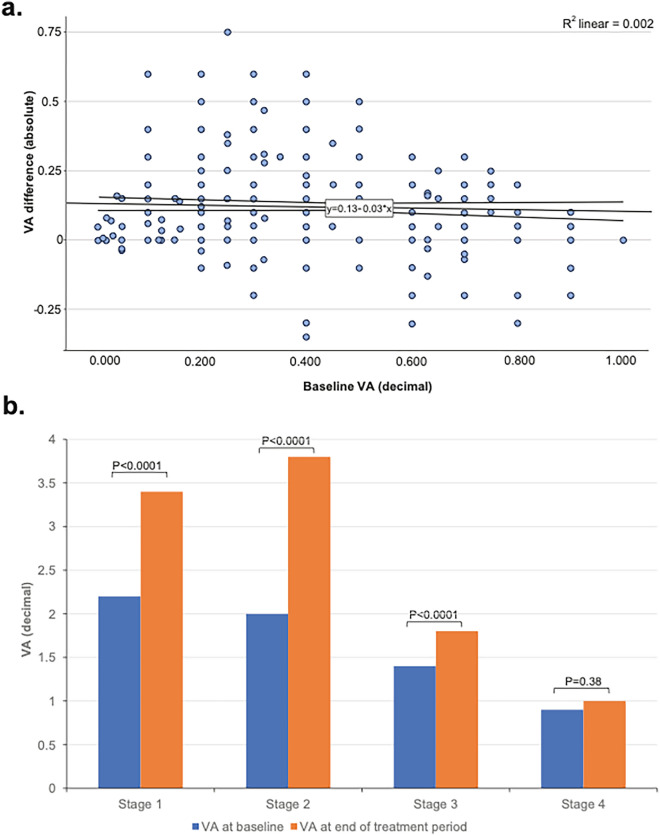
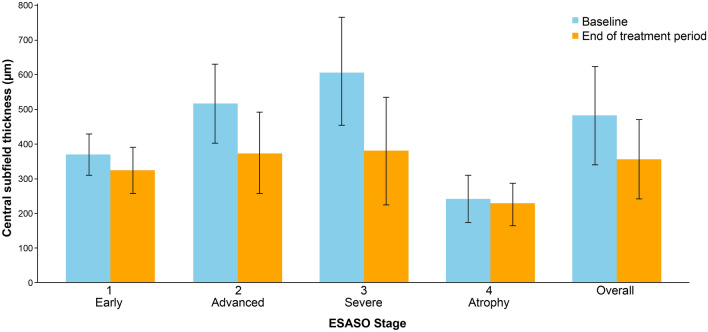
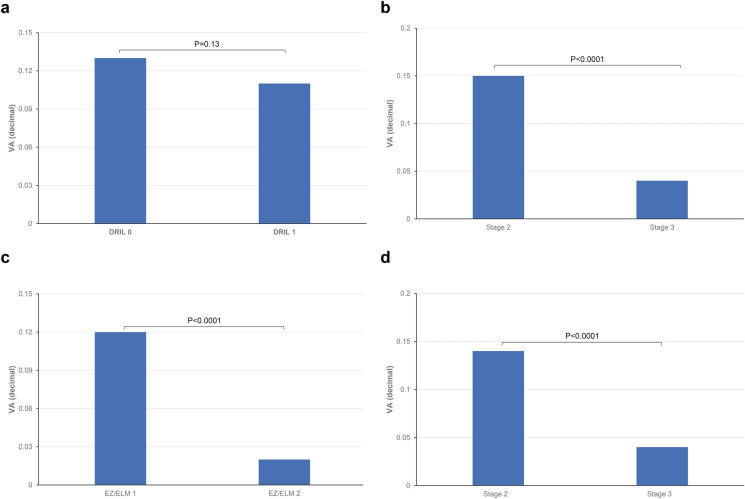
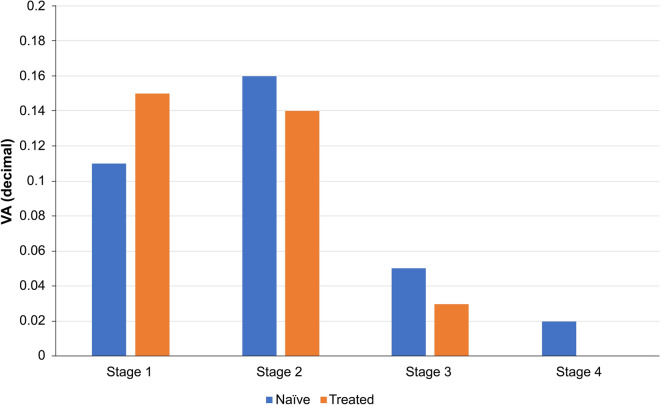
Results: Of the 560 eyes studied (62% male, mean age 66.7 years), 31% were classified as stage 1 (early), 50% stage 2 (advanced), 17% stage 3 (severe), and 2% stage 4 (atrophic). Visual acuity (VA; decimal) improved by 0.12-0.15 decimals in stages 1-2 but only 0.03 decimal in stage 3 (all p < 0.0001) and 0.01 in stage 4 (p = 0.38). Even in eyes with low baseline VA ≤ 0.3, improvements were significant only in stages 1 and 2 (0.12 and 0.17 decimals, respectively). Central subfield thickness (CST) improvement was greatest in stage 3 (-229 µm, 37.6%, p < 0.0001), but uncorrelated with VA gains, unlike stages 1 and 2 (respectively: -142 µm, 27.4%; - 5 µm, 12%; both p < 0.0001). Stage 4 showed no significant CST change. Baseline disorganization of retinal inner layers and focal damage of the ellipsoid zone/external limiting membrane did not influence VA improvement in stages 1 and 2. Treatment patterns varied, with 61% receiving anti-VEGF and 39% dexamethasone, influenced by DME stage, with no significant differences between therapeutic agents.
Conclusion: The ESASO classification, which views the retina as a neurovascular unit and integrates multiple biomarkers, surpasses single biomarkers in predicting visual outcomes. Significant functional improvement occurred only in stages 1 and 2, suggesting reversible damage, whereas stages 3 and 4 likely reflect irreversible damage.
Keywords: Anti-VEGF; Diabetic macular edema; ESASO classification; OCT Biomarkers; Optical coherence tomography; Retinal Neurovascular Unit; Steroid; Treatment outcomes in DME.
© 2024. The Author(s).
Conflict of interest statement
Neither Giacomo Panozzo nor Maria Vittoria Cicinelli, Giulia Dalla Mura, Diana Giannarelli, Maria Vadalà, Vincenza Bonfiglio, Giovanni Bellisario, nor Francesco Bandello received financial support for the research,authorship, and/or publication of this article.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas Ninth Edition. 2019.
-
- Panozzo G, Cicinelli MV, Augustin AJ, et al. An optical coherence tomography-based grading of diabetic maculopathy proposed by an international expert panel: the European School for Advanced Studies in Ophthalmology classification. Eur J Ophthalmol. 2020;30(1):8–18. doi: 10.1177/1120672119880394. - DOI - PubMed
LinkOut - more resources
Full Text Sources
