

Continuous stellate ganglion block for ventricular arrhythmias: case series, systematic review, and differences from thoracic epidural anaesthesia
- PMID: 38531027
- PMCID: PMC11020261
- DOI: 10.1093/europace/euae074
Continuous stellate ganglion block for ventricular arrhythmias: case series, systematic review, and differences from thoracic epidural anaesthesia
Abstract
Aims: Percutaneous stellate ganglion block (PSGB) through single-bolus injection and thoracic epidural anaesthesia (TEA) have been proposed for the acute management of refractory ventricular arrhythmias (VAs). However, data on continuous PSGB (C-PSGB) are scant. The aim of this study is to report our dual-centre experience with C-PSGB and to perform a systematic review on C-PSGB and TEA.
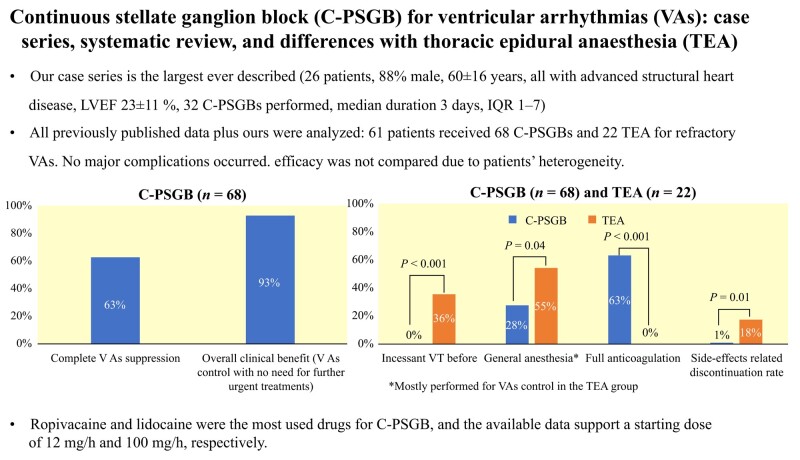
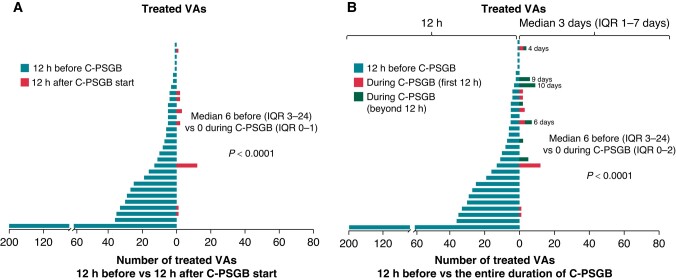
Methods and results: Consecutive patients receiving C-PSGB at two centres were enrolled. The systematic literature review follows the latest Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria. Our case series (26 patients, 88% male, 60 ± 16 years, all with advanced structural heart disease, left ventricular ejection fraction 23 ± 11%, 32 C-PSGBs performed, with a median duration of 3 days) shows that C-PSGB is feasible and safe and leads to complete VAs suppression in 59% and to overall clinical benefit in 94% of cases. Overall, 61 patients received 68 C-PSGBs and 22 TEA, with complete VA suppression in 63% of C-PSGBs (61% of patients). Most TEA procedures (55%) were performed on intubated patients, as opposed to 28% of C-PSGBs (P = 0.02); 63% of cases were on full anticoagulation at C-PSGB, none at TEA (P < 0.001). Ropivacaine and lidocaine were the most used drugs for C-PSGB, and the available data support a starting dose of 12 and 100 mg/h, respectively. No major complications occurred, yet TEA discontinuation rate due to side effects was higher than C-PSGB (18 vs. 1%, P = 0.01).
Conclusion: Continuous PSGB seems feasible, safe, and effective for the acute management of refractory VAs. The antiarrhythmic effect may be accomplished with less concerns for concomitant anticoagulation compared with TEA and with a lower side-effect related discontinuation rate.
Keywords: Cardiac arrest; Electrical storm; Neuromodulation; Refractory ventricular arrhythmias; Stellate ganglion block; Thoracic epidural anaesthesia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures
References
-
- Elsokkari I, Parkash R, Tang A, Wells G, Doucette S, Yetisir E et al. Mortality risk increases with clustered ventricular arrhythmias in patients with implantable cardioverter-defibrillators. JACC Clin Electrophysiol 2020;6:327–37. - PubMed
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Yanowitz F, Preston JB, Abildskov JA. Functional distribution of right and left stellate innervation to the ventricles. Production of neurogenic electrocardiographic changes by unilateral alteration of sympathetic tone. Circ Res 1966;18:416–28. - PubMed
-
- Schwartz PJ, Snebold NG, Brown AM. Effects of unilateral cardiac sympathetic denervation on the ventricular fibrillation threshold. Am J Cardiol 1976;37:1034–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
