

Polygenic risk score for ulcerative colitis predicts immune checkpoint inhibitor-mediated colitis
- PMID: 38531883
- PMCID: PMC10966072
- DOI: 10.1038/s41467-023-44512-4
Polygenic risk score for ulcerative colitis predicts immune checkpoint inhibitor-mediated colitis
Abstract
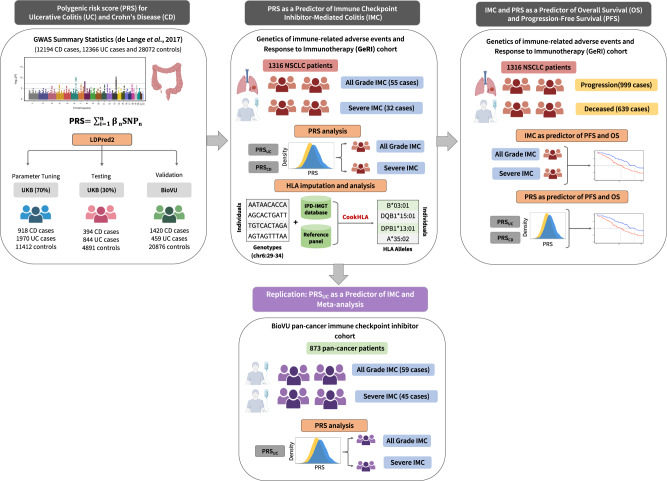
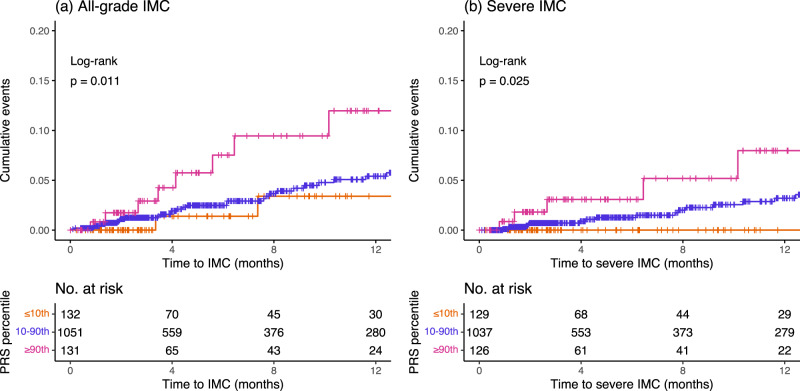
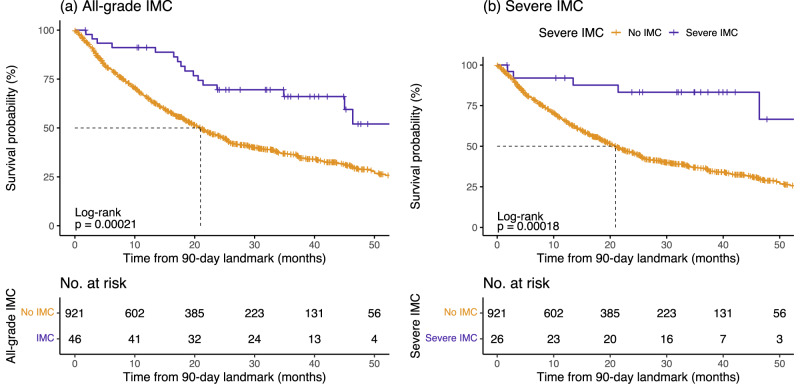
Immune checkpoint inhibitor-mediated colitis (IMC) is a common adverse event of treatment with immune checkpoint inhibitors (ICI). We hypothesize that genetic susceptibility to Crohn's disease (CD) and ulcerative colitis (UC) predisposes to IMC. In this study, we first develop a polygenic risk scores for CD (PRSCD) and UC (PRSUC) in cancer-free individuals and then test these PRSs on IMC in a cohort of 1316 patients with ICI-treated non-small cell lung cancer and perform a replication in 873 ICI-treated pan-cancer patients. In a meta-analysis, the PRSUC predicts all-grade IMC (ORmeta=1.35 per standard deviation [SD], 95% CI = 1.12-1.64, P = 2×10-03) and severe IMC (ORmeta=1.49 per SD, 95% CI = 1.18-1.88, P = 9×10-04). PRSCD is not associated with IMC. Furthermore, PRSUC predicts severe IMC among patients treated with combination ICIs (ORmeta=2.20 per SD, 95% CI = 1.07-4.53, P = 0.03). Overall, PRSUC can identify patients receiving ICI at risk of developing IMC and may be useful to monitor patients and improve patient outcomes.
© 2024. The Author(s).
Conflict of interest statement
J.M.B. receives research support from Genentech/Roche and Incyte Corporation, has received advisory board payments from AstraZeneca and Mallinckrodt, and is an inventor on patents regarding immunotherapy targets and biomarkers in cancer. The remaining authors declare no other competing interests.
Figures
Update of
-
Polygenic risk score for ulcerative colitis predicts immune checkpoint inhibitor-mediated colitis.medRxiv [Preprint]. 2023 Sep 13:2023.05.15.23289680. doi: 10.1101/2023.05.15.23289680. medRxiv. 2023. Update in: Nat Commun. 2024 Mar 26;15(1):2568. doi: 10.1038/s41467-023-44512-4. PMID: 37292751 Free PMC article. Updated. Preprint.
References
-
- Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discov. 2018;8:1069–1086. doi: 10.1158/2159-8290.CD-18-0367. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- S10 OD017985/OD/NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- R01 CA227466/CA/NCI NIH HHS/United States
- T32 CA009207/CA/NCI NIH HHS/United States
- S10 RR025141/RR/NCRR NIH HHS/United States
- R01 CA251758/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- UG1 CA233259/CA/NCI NIH HHS/United States
- R01 CA227481/CA/NCI NIH HHS/United States
- R01 HD074711/HD/NICHD NIH HHS/United States
- RC2 GM092618/GM/NIGMS NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- U01 HG006378/HG/NHGRI NIH HHS/United States
- K24 CA169004/CA/NCI NIH HHS/United States
- P01 CA129243/CA/NCI NIH HHS/United States
- U01 CA253560/CA/NCI NIH HHS/United States
- U19 HL065962/HL/NHLBI NIH HHS/United States
- R01 HL156021/HL/NHLBI NIH HHS/United States
- K12 DK133995/DK/NIDDK NIH HHS/United States
- P50 GM115305/GM/NIGMS NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- R01 NS032830/NS/NINDS NIH HHS/United States
- U01 HG004798/HG/NHGRI NIH HHS/United States
- R01 CA276266/CA/NCI NIH HHS/United States
