

Evaluation of the deliverability of dynamic conformal arc therapy (DCAT) by gantry wobble and its influence on dose
- PMID: 38532018
- PMCID: PMC10965989
- DOI: 10.1038/s41598-024-57644-4
Evaluation of the deliverability of dynamic conformal arc therapy (DCAT) by gantry wobble and its influence on dose
Abstract
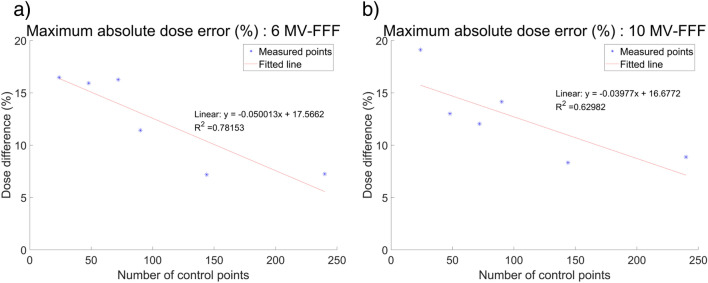
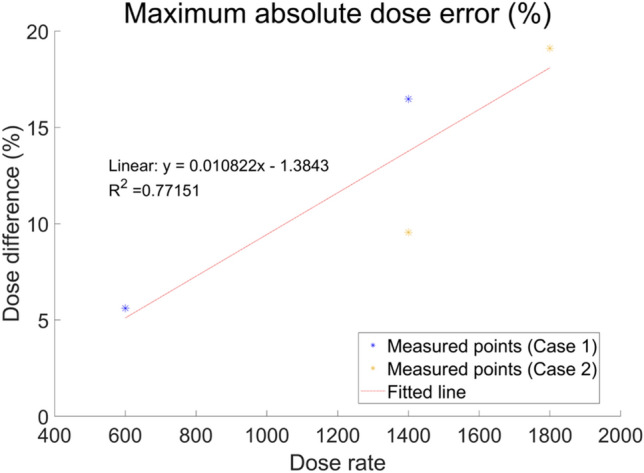
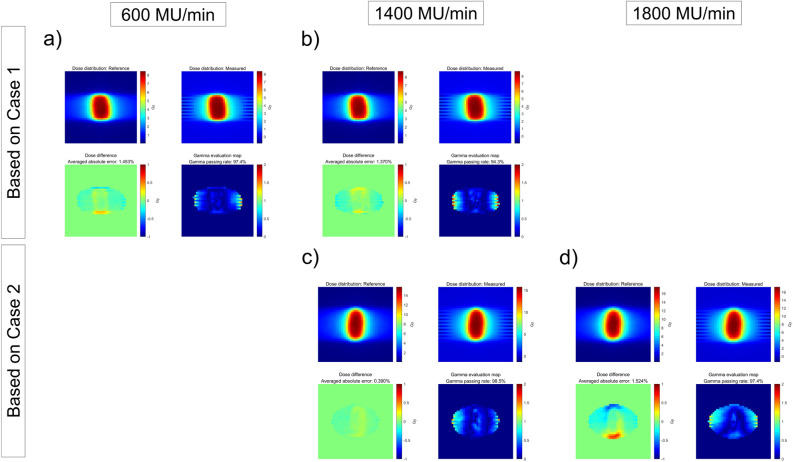
We aimed to investigate the deliverability of dynamic conformal arc therapy (DCAT) by gantry wobble owing to the intrinsic inter-segment break of the Elekta linear accelerator (LINAC) and its adverse influence on the dose to the patient. The deliverability of DCAT was evaluated according to the plan parameters, which affect the gantry rotation speed and resultant positional inaccuracies; the deliverability according to the number of control points and dose rates was investigated by using treatment machine log files and dosimetry devices, respectively. A non-negligible degradation in DCAT deliverability due to gantry wobble was observed in both the treatment machine log files and dosimetry devices. The resulting dose-delivery error occurred below a certain number of control points or above a certain dose rate. Dose simulations in the patient domain showed a similar impact on deteriorated deliverability. For targets located primarily in the isocenter, the dose differences were negligible, whereas for organs at risk located mainly off-isocenter, the dose differences were significant up to - 8.77%. To ensure safe and accurate radiotherapy, optimal plan parameters should be selected, and gantry angle-specific validations should be conducted before treatment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Effects of collimator angle, couch angle, and starting phase on motion-tracking dynamic conformal arc therapy (4D DCAT).J Appl Clin Med Phys. 2017 Sep;18(5):54-63. doi: 10.1002/acm2.12132. Epub 2017 Jul 21. J Appl Clin Med Phys. 2017. PMID: 28730652 Free PMC article.
-
Texture analysis on the fluence map to evaluate the degree of modulation for volumetric modulated arc therapy.Med Phys. 2014 Nov;41(11):111718. doi: 10.1118/1.4897388. Med Phys. 2014. PMID: 25370632
-
A dosimetric comparison of three-dimensional conformal radiotherapy, volumetric-modulated arc therapy, and dynamic conformal arc therapy in the treatment of non-small cell lung cancer using stereotactic body radiotherapy.J Appl Clin Med Phys. 2014 Sep 8;15(5):4898. doi: 10.1120/jacmp.v15i5.4898. J Appl Clin Med Phys. 2014. PMID: 25207575 Free PMC article.
-
Dynamic conformal arc therapy: transmitted signal in vivo dosimetry.Med Phys. 2008 May;35(5):1830-9. doi: 10.1118/1.2900718. Med Phys. 2008. PMID: 18561658
-
Treating lung cancer with dynamic conformal arc therapy: a dosimetric study.Radiat Oncol. 2017 Jun 2;12(1):93. doi: 10.1186/s13014-017-0823-y. Radiat Oncol. 2017. PMID: 28578699 Free PMC article.
Cited by
-
A volumetric modulated arc therapy-based dynamic conformal arc technique with limited monitor units (VMATliMU) to reduce multileaf collimator interplay effects: A computational phantom study for stage I non-small-cell lung cancer.PLoS One. 2025 Sep 9;20(9):e0332190. doi: 10.1371/journal.pone.0332190. eCollection 2025. PLoS One. 2025. PMID: 40924712 Free PMC article.
-
Dosimetric and radiobiological evaluation of stereotactic radiosurgery using volumetric modulated arc therapy and dynamic conformal arc therapy for multiple brain metastases.Sci Rep. 2025 Mar 17;15(1):9118. doi: 10.1038/s41598-025-93502-7. Sci Rep. 2025. PMID: 40097578 Free PMC article.
-
Effects of Differences in the Increment Parameter Controlling Sector Numbers on Volumetric-Modulated Arc-Based Radiosurgery Planning With the Monaco® System for Single Brain Metastases.Cureus. 2025 Jan 12;17(1):e77324. doi: 10.7759/cureus.77324. eCollection 2025 Jan. Cureus. 2025. PMID: 39935917 Free PMC article.
References
-
- Rudra S, et al. High dose adaptive MRI guided radiation therapy improves overall survival of inoperable pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017;99:E184. doi: 10.1016/j.ijrobp.2017.06.1042. - DOI
-
- Saglam Y, Selek U, Bolukbasi Y. A novel and clinically useful weight-optimized dynamic conformal arc in stereotactic radiation therapy of non-small cell lung cancer: Dosimetric comparison of treatment plans with volumetric-modulated arc therapy. Radiat. Phys. Chem. 2023;203:110623. doi: 10.1016/j.radphyschem.2022.110623. - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
