

Right ventricular injury in patients with COVID-19-related ARDS eligible for ECMO support: a multicenter retrospective study
- PMID: 38532049
- PMCID: PMC10965859
- DOI: 10.1186/s13613-024-01256-8
Right ventricular injury in patients with COVID-19-related ARDS eligible for ECMO support: a multicenter retrospective study
Abstract
Background: Coronavirus disease 2019 (COVID-19)-related acute respiratory distress syndrome (ARDS) is associated with high mortality. Extracorporeal membrane oxygenation (ECMO) has been proposed in this setting, but optimal criteria to select target patients remain unknown. Our hypothesis is that evaluation of right ventricular (RV) function could be helpful. The aims of our study were to report the incidence and outcomes of patients eligible for ECMO according to EOLIA criteria, and to identify a subgroup of patients with RV injury, which could be a target for ECMO.
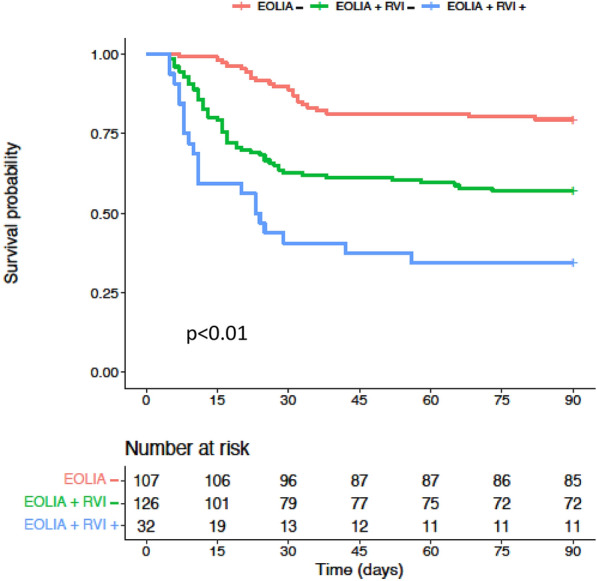
Methods: Retrospective observational study involving 3 French intensive care units (ICUs) of teaching hospitals. Patients with confirmed SARS-CoV-2 infection between March 2020 and March 2021, presenting ARDS and with available echocardiography, were included. Patients were classified in three groups according to whether or not they met the EOLIA criteria and the presence of RV injury (RVI) ("EOLIA -", "EOLIA + RVI -" and "EOLIA + RVI + "). RVI was defined by the association of RV to left ventricular end-diastolic area ratio > 0.8 and paradoxical septal motion. Kaplan-Meier survival curves were used to analyze outcome as well as a Cox model for 90 day mortality.
Results: 915 patients were hospitalized for COVID-19, 418 of them with ARDS. A total of 283 patients with available echocardiography were included. Eighteen (6.3%) patients received ECMO. After exclusion of these patients, 107 (40.5%) were classified as EOLIA -, 126 (47.5%) as EOLIA + RVI -, and 32 (12%) as EOLIA + RVI + . Ninety-day mortality was 21% in the EOLIA-group, 44% in the EOLIA + RVI-group, and 66% in the EOLIA + RVI + group (p < 0.001). After adjustment, RVI was statistically associated with 90-day mortality (HR = 1.92 [1.10-3.37]).
Conclusions: Among COVID-19-associated ARDS patients who met the EOLIA criteria, those with significant RV pressure overload had a particularly poor outcome. This subgroup may be a more specific target for ECMO. This represented 12% of our cohort compared to 60% of patients who met the EOLIA criteria only. How the identification of this high-risk subset of patients translates into patient-centered outcomes remains to be evaluated.
Keywords: Acute respiratory distress syndrome; COVID-19; Extracorporeal membrane oxygenation; Right ventricle.
© 2024. The Author(s).
Conflict of interest statement
AVB reports personal fees from Air Liquide for clinical research. PV gave a lecture at a Baxter symposium during the 2022 SRLF congress.
Figures


References
-
- Barbaro RP, MacLaren G, Boonstra PS, Iwashyna TJ, Slutsky AS, Fan E, et al. Extracorporeal membrane oxygenation support in COVID-19: an international cohort study of the extracorporeal life support organization registry. Lancet Lond Engl. 2020;396(10257):1071–1078. doi: 10.1016/S0140-6736(20)32008-0. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
