

ATP releasing channels and the ameliorative effects of high intensity interval training on diabetic heart: a multifaceted analysis
- PMID: 38532054
- PMCID: PMC10965991
- DOI: 10.1038/s41598-024-57818-0
ATP releasing channels and the ameliorative effects of high intensity interval training on diabetic heart: a multifaceted analysis
Abstract
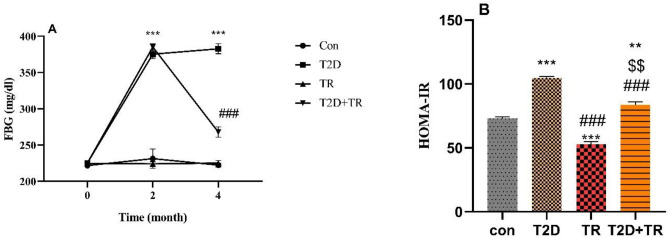
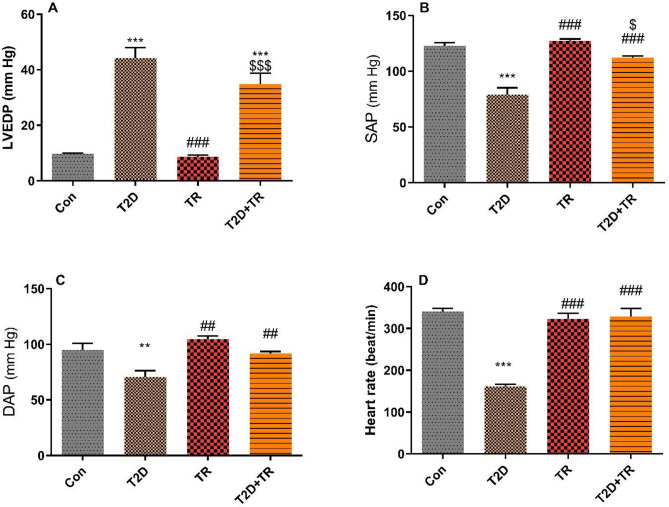
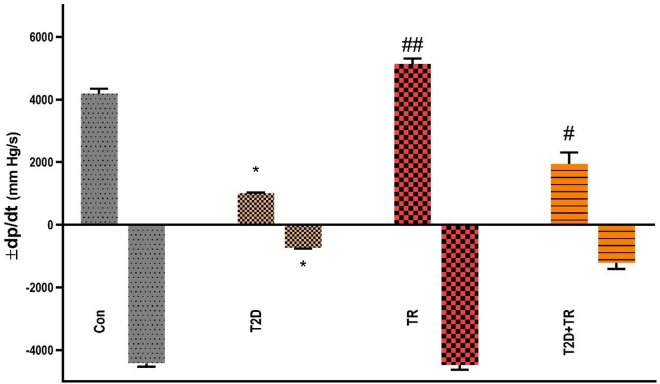
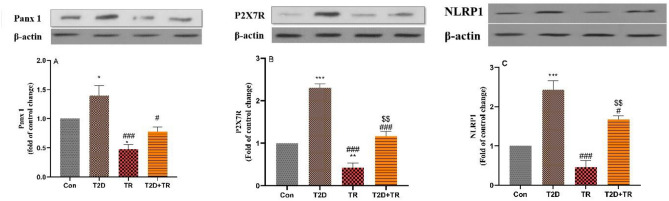
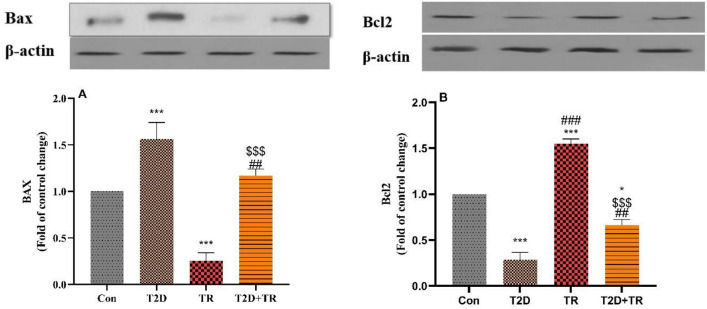
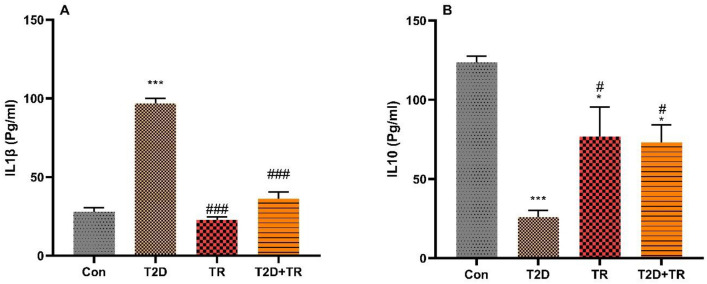
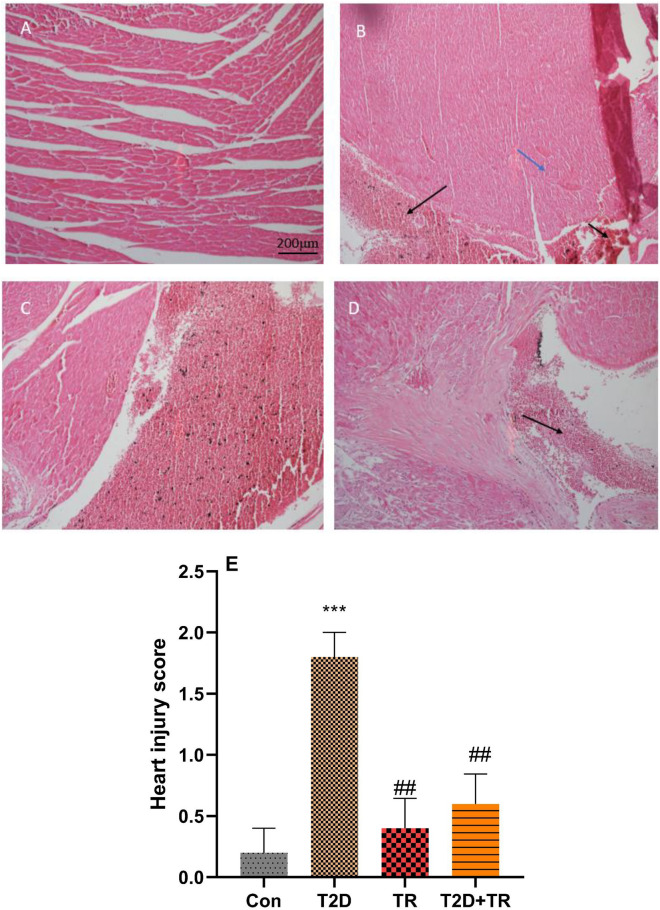
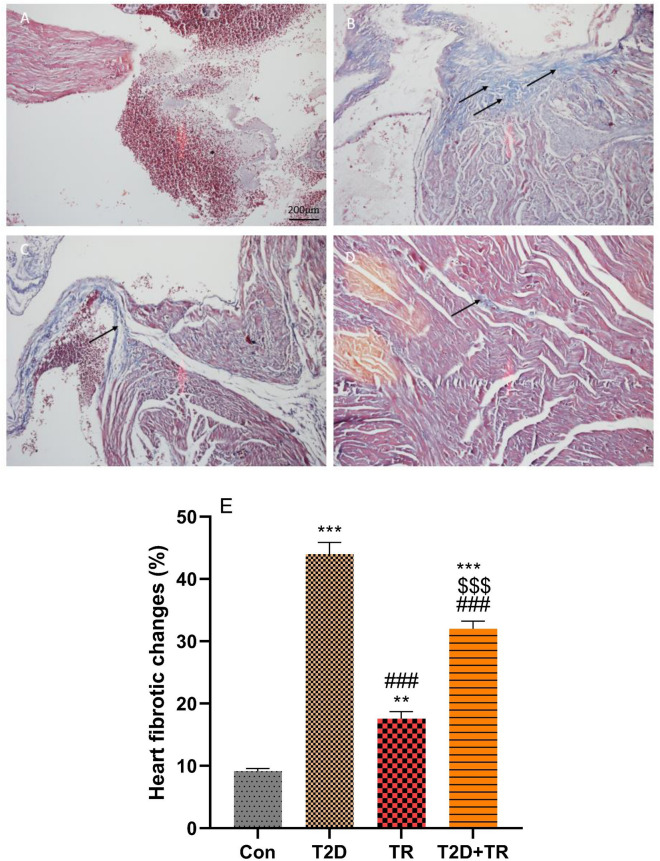
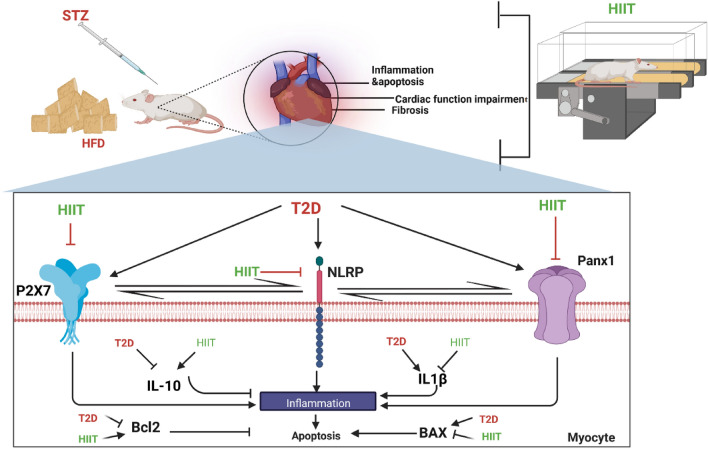
Type 2 diabetes (T2D) can cause severe cardiac complications at functional, histologic and molecular levels. These pathological complications could be mediated by ATP-releasing channels such as Panx1 and ATP receptors, in particular P2X7. The aim of our study was to investigate the effect of high-intensity interval training (HIIT) on T2D-induced cardiac complications at the functional, histopathological and molecular levels, with a particular focus on ATP-releasing channels. 48 male Wistar rats at the age of 8 weeks were randomly allocated into four groups: control (Con), Diabetes (T2D), Training (TR), and Diabetes + Training (T2D + TR). T2D was induced by a high-fat diet plus a low dose (35 mg/kg) of STZ administration. Rats in the TR and T2D + TR groups underwent an 8-weeks training program involving intervals ranging from 80 to 100% of their maximum running speed (Vmax), with 4-10 intervals per session. Protein expression of Interleukin 1β (IL1β), Interleukin 10 (IL-10), Pannexin 1 (Panx1), P2X7R (purinergic P2X receptor 7), NLRP1 (NLR Family Pyrin Domain Containing 1), BAX, and Bcl2 were measured in the heart tissue. Additionally, we assessed heart function, histopathological changes, as well as insulin resistance using the homeostasis model assessment of insulin resistance (HOMA-IR). In contrast to the T2D group, HIIT led to increased protein expression of Bcl2 and IL-10 in the heart. It also resulted in improvements in systolic and diastolic blood pressures, heart rate, ± dp/dt (maximum and minimum changes in left ventricular pressure), while reducing protein expression of IL-1β, Panx1, P2X7R, NLRP1, and BAX levels in the heart. Furthermore, left ventricular diastolic pressure (LVDP) was reduced (P ≤ 0.05). Moreover, heart lesion scores increased with T2D but decreased with HIIT, along with a reduction in fibrosis percentage (P ≤ 0.05). The results of this study suggest that the cardioprotective effects of HIIT on the diabetic heart may be mediated by the modulation of ATP-releasing channels. This modulation may lead to a reduction in inflammation and apoptosis, improve cardiac function, and attenuate cardiac injury and fibrosis.
Keywords: ATP-releasing channels; HIIT; Inflammation; Type 2 diabetes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
High-Intensity Interval Training Ameliorates Molecular Changes in the Hippocampus of Male Rats with the Diabetic Brain: the Role of Adiponectin.Mol Neurobiol. 2023 Jun;60(6):3486-3495. doi: 10.1007/s12035-023-03285-z. Epub 2023 Mar 6. Mol Neurobiol. 2023. PMID: 36877358
-
Lung molecular and histological changes in type 2 diabetic rats and its improvement by high-intensity interval training.BMC Pulm Med. 2024 Jan 17;24(1):37. doi: 10.1186/s12890-024-02840-1. BMC Pulm Med. 2024. PMID: 38233819 Free PMC article.
-
Potential Role of High-Intensity Interval Training-Induced Increase in Humanin Levels for the Management of Type 2 Diabetes.J Cell Mol Med. 2025 Feb;29(3):e70396. doi: 10.1111/jcmm.70396. J Cell Mol Med. 2025. PMID: 39936487 Free PMC article.
-
The Combined Effect of High-Intensity Interval Training and Time-Restricted Feeding on the AKT-IGF-1-mTOR Signaling Pathway in the Muscle Tissue of Type 2 Diabetic Rats.Nutrients. 2025 Apr 22;17(9):1404. doi: 10.3390/nu17091404. Nutrients. 2025. PMID: 40362714 Free PMC article.
-
High-Intensity Interval Training in Patients with Type 2 Diabetes Mellitus: a Systematic Review.Curr Atheroscler Rep. 2019 Feb 2;21(2):8. doi: 10.1007/s11883-019-0767-9. Curr Atheroscler Rep. 2019. PMID: 30712240
Cited by
-
Effects of high-intensity interval training on metabolic impairments in liver tissue of rats with type 2 diabetes: a metabolomics-based approach.J Physiol Biochem. 2025 Aug;81(3):611-624. doi: 10.1007/s13105-025-01085-8. Epub 2025 May 16. J Physiol Biochem. 2025. PMID: 40377860
-
Changes in the hippocampal level of tau but not beta-amyloid may mediate anxiety-like behavior improvement ensuing from exercise in diabetic female rats.Behav Brain Funct. 2024 May 3;20(1):9. doi: 10.1186/s12993-024-00235-0. Behav Brain Funct. 2024. PMID: 38702776 Free PMC article.
-
High-intensity interval training reduces Tau and beta-amyloid accumulation by improving lactate-dependent mitophagy in rats with type 2 diabetes.Iran J Basic Med Sci. 2024;27(11):1430-1439. doi: 10.22038/ijbms.2024.77038.16664. Iran J Basic Med Sci. 2024. PMID: 39386233 Free PMC article.
-
The effect of high-intensity interval training on type 2 diabetic muscle: A metabolomics-based study.Heliyon. 2024 Jul 20;10(15):e34917. doi: 10.1016/j.heliyon.2024.e34917. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39170342 Free PMC article.
-
Various endurance training intensities improve GFR and Up-regulate AQP2/GSK3β in lithium-induced nephropathic rats.BMC Nephrol. 2025 Feb 6;26(1):60. doi: 10.1186/s12882-025-03997-5. BMC Nephrol. 2025. PMID: 39915719 Free PMC article.
References
-
- Rami M, Azimpour M, Khoramipour K. The effect of 8 weeks of High Intensity Interval Training on the Levels of Wnt and NF-κB proteins in the heart tissue of male Wistar rats with type 2 diabetes. J. Sport Exercise Physiol. 2023;15(4/19):30.
-
- Rajizadeh MA, et al. Investigating the effects of Citrullus colocynthis on cognitive performance and anxiety-like behaviors in STZ-induced diabetic rats. Int. J. Neurosci. 2021;133:1–13. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
